Contents
Acronyms
USAID - United States Agency for International Development
FHI - Family Health International
IMPACT - Implementing AIDS Prevention and Care Project
NACO - National AIDS Control Organization, New Delhi, India
NSACS - Nagaland State AIDS Control Society, Kohima, Nagaland
PLHA - People Living with HIV/AIDS
ECS - Elutheros Christian Society, Tuensang, Nagaland
VCTC - Voluntary Counseling and Testing Center (For HIV)
PPTCT - Prevention of Parent to Child Transmissions (PMTCT)
IDU - Injecting Drug User(s) / Use
STI - Sexually Transmitted Infections
RTI - Reproductive Tract Infections
UTI - Urinary Tract Infections
SHG - Self Help Group(s)
ANC - Ante-Natal Clinic (s) / attendees
No. 4 - Commonly Available Heroin quality in Tuensang district
SP - Spasmo Proxyvon abused orally as well as diluted & injected
ADC - Additional Deputy Commissioner
SDO - Sub-Divisional Officer
EAC - Extra Assistant Commissioner
NGO - Non Governmental organizations (Non Profit/Voluntary)
OVC - Orphans and Vulnerable Children
HRG - High Risk Groups
TMPO - Tuensang Mon People’s Organisation.
TMSF - Tuensang Mon Students Federation.
KBCA - Khiamniungan Baptist Churches Association.
CKS - Chang Khulie Setchang (Chang Tribal Council.
TTBWU - Tuensang Town Baptist Women Union.
KTC - Khiamniungan Tribal Council
USLB - Sangtam tribal Council.
PBCA - Phom Baptist Churches Association
PH - Phomla Hoichem( Apex Body of the Phom women).
SBC - Shamator Baptist Church.
CACS - Churches Alliance for Community Support.
SBC - Sangtam Baptist Church.
MLA - Member of Legislative Assembly.
GB - Goan Bura (Offically appointed local law enforcer)
DB - Dobashi (Govt. appointed Interpreter)
SDO - Sub Divisional Officer.
DIS - Deputy Inspector of Schools.
TTABC - Tuensang Town Ao Baptist Church.
DTO - District Tuberculosis Officer.
NAP - Nagaland Armed Police:
TTPU - Tuensang Town Pastors Union.
TTBC - Tuensang Town Baptist Church.
DACC - Tuensang District AIDS Control Committee.
HC - Hindu Community.
MC - Muslim community.
Executive Summary
Gunashekar working on this section after the following:
- 1. Revising content, language, accuracy of each section
1. Introduction
1.1 Background
The National AIDS Control Organization (NACO) in India estimated that 3.82 to 4.58 million people in the country were living with HIV/AIDS by the year 2002. The state Nagaland was classified as one of the six high prevalence states in India with over one percent of pregnant women testing positive for HIV. HIV is no longer limited to High Risk Groups. It affects everyone. Of the 49 high prevalence HIV/AIDS districts in the country, three are in Nagaland. HIV prevalence among Injecting Drug Users was found to be 10.3% (NACO 2002) in Nagaland.
The District Tuensang reported very high prevalence figures both among the General Population group of Pregnant Women (8% - NACO 2002) and among Injecting Drug Users (24.6% - NACO 2002).
Tuensang district is grappling with the twin issues of substance abuse and HIV/AIDS among its communities. The district shares a 159 Km long border with Myanmar (Burma) and is close to the area known as the ‘Golden Triangle ‘ – an area infamous for production and supply of heroin and opium throughout South Asia.

While there are some efforts at HIV prevention and care in the district by the government and the voluntary sector in the district, there is an urgent need for an expanded comprehensive prevention to care response in Tuensang district.
The Elutheros Christian Society (ECS) is among the most active organizations in Tuensang district working on HIV/AIDS prevention care and support issues. In partnership with the Nagaland State AIDS Control Society and with technical support from Family Health International (FHI), ECS has carried out this comprehensive assessment of the situation and responses in the district.
This work was supported by the U.S. Agency for International Development (USAID) through Family Health International’s Implementing AIDS Prevention and Care (IMPACT) Project.
The assessment will contribute to planning an expanded comprehensive response in the high prevalence district. Similar efforts are being carried out by FHI in other High Prevalence Districts in India. This report presents the findings of the assessment in Tuensang District.
Tuensang was earlier a part of what the British called North East Frontier Agency and remained the largest district of Nagaland till the beginning of 2004 since when three smaller districts are being carved out of Tuensang district. For the purpose of this study the older and larger district is being considered as the assessment area.
More than 6 different tribes live in this frontier district. What unites them is perhaps their faith in Christianity though they speak different languages and have their own churches and collective opinions. This report also attempts to provide a picture of environmental differences and similarities between these communities.
- 1.2 Goal and Strategies
The Goal of the exercise was to conduct a comprehensive situational assessment of HIV/AIDS and current responses in Tuensang District in Nagaland. The assessment strategies used were:
Situation: Assessment of the current scenario and dynamics of the epidemic.
Response: Assessment of the current efforts by different sectors to address this epidemic
Needs: Identification of specific needs of the community through participatory consultative processes.
Resources: Mapping of existing community resources. And …
Action: Consensus building on prioritized needs, current responses and possible actions.
Each of the above strategies has been analyzed in separate sections of this report. The remaining part of this section explains the assessment process and provides a profile of the study area in terms of the Physical, Political, Economic, Social, Cultural, Health and Medical Environments.
- 1.3 Assessment Process
The assessment team was an interesting combination of ECS counselors, recovered drug users, PLHA, researchers and a representative of NSACS.
FHI provided the services of technical consultant who has the experience of planning and guiding similar assessments. The Technical consultant oriented the ECS team on the assessment and helped plan the activities. The field work was planned in 5 locations across the district. (Tuensang town, Shamator, Noklak, Kiphirie and Longleng)
Available secondary material was collected from the NSACS office at Kohima, Civil Hospital Tuensang, VCTC and PPTC data available within ECS, various government department annual reports and brief reports.
Primary information was collected through a structured interview among 500 respondents spread across different church congregations of different tribes. This was to understand ‘Stigma and discrimination’ in Tuensang Town.
Another rapid survey of different types of outlets was conducted at 3 locations including Tuensang town. This was to find condom sources in the open market.
The focus of the assessment however was qualitative in depth interviews, group discussions, and consultative meetings with stakeholders and community members individually and in groups. Participative methods were used in group discussions to identify specific community needs and understand different perceptions..
The transcripts of the qualitative assessments and field reports were translated into English as each tribe spoke a different language. The content was analyzed using manual content analysis procedures. The structured interviews were analyzed using spreadsheet software and the rapid assessment findings were summarized by the field team members.
The key findings from the exercise were shared and discussed with a consultative meeting of different stakeholders and further inputs were obtained. This meeting also initiated the consensus building process among the communities.
- 1.4 Profile of ECS
The threat of drugs took its toll on the young population as early as the late 1980’s. Death knocked almost every household and the impact of drugs left many families to grapple with the intensity of having lost young sons and daughters to the menace of heroin, known as No.4 in the community. The close proximity with one of the infamous “Golden Triangle” countries, Myanmar posed a major threat to the general population as the district saw emergence of HIV/AIDS cases as early as the 1990’s. The tribal communities inhabited both side of the International border and this made it conducive for peddlers who stalked the area in the guise of merchants, porters, well-wishers and peddled ‘Heroin No. 4’. Tuensang district became a major transit point for inflow of high quality ‘Heroin’ into other parts of the country.
The adverse impact of drugs led to formation of the Eleutheros Christian Society in the year 1992 December. ECS was registered on March 1993 under the Society Registered Act 1860 and FRCA (Foreign Contributions Regulations Act 1976) on 9th January, 1998. In Greek’ the word ‘eleutheros’ means “Freed one” thus giving the organization the vision to address one of the most challenging issues that have confronted a tribal community that has a population of 414,810. The organization was formed to make concerted effort to wean away youth population and aimed at social integration through intensive awareness and intervention in the targeted population. Emergence of HIV/AIDS painted yet another grim picture as the organization was faced with the challenge of premature deaths among recovered drug users.
ECS was known initially for its Rehabilitation efforts for drug users/alcoholics, but later extended to other efforts in poverty eradication programmes. ECS drew its initial inspiration from growing drug user deaths. All efforts were invested to create an enabling environment to break-through and reach gangs, users and peddlers.
The organization spent tremendous efforts in rapport building among clients, families and relatives. Counseling services for HIV/AIDS was initiated in the year 1993; Narcotic Anonymous and SHG were formed to created support for IDU. Capacity building of staff was the focus of intervention and four staff members were trained at the “Christian Institute for Transformation Ministry in Hong Kong during this phase. The District Planning Board of Tuensang supported the organization and a Rehabilitation Centre “House of Hope” was established at ‘Longpang’ 27 km from the district headquarters and the first batch of 16 IDU were recruited on 6th April 1995. ‘Every Home Intervention’ programme on HIV/AIDS gained its momentum and IEC and Outreach services were strengthened during this period. Education establishments were targeted for providing information on Drugs and HIV/AIDS and led to the formation of ‘Core Groups’ for peer support and services to addicted students.
The symptomatic addressing of Drug problem in the district was yielding no results as more deaths defied intense intervention by the community. This led to a comprehensive policy to involve community stakeholders and reducing demand among drug users as well as supply reduction of drugs to and from the district.
1.5 Profile of Tuensang
Located at the northeastern corner of the state of Nagaland the Tuensang district shares 159 kilometers long border with Myanmar (Burma) in the east, Mon district in the north, Assam in the northwest, Mokokchung and Zunheboto districts in the west and Phek district in the south. Tuensang was a part of the area earlier known as North-East Frontier Agency (NEFA).
Satellite Map of Tuensang District

In 1957 Tuensang division of the then NEFA became a district as one of the then three districts of the state viz. Kohima, Mokokchung and Tuensang. In December 1963 the district of Nagaland was divided into seven districts in place of three. Tuensang district had an area of 4,228 sq. km until recently, the district has been further divided into three districts viz. Tuensang district, Kiphire district and Longleng district since January 24th 2004.
1.5.1 Physical Environment
Tuensang district spreads over 4228 square kilometers. Tuensang district is a small version of Nagaland with six different tribes; Chang, Yimchunger, Khiamniungan, Sangtam, Phom and Sumi.

1.5.1.1. Tuensang Town
Tuensang town is located at an altitude of 1371.60 meters above sea level and the entire area is divided into high hill areas and lower hill areas. The topography of the region is very severe, with steep hill ranges that break into a wide chaos of rugged ridges. It is situated on 26 degrees-49 degree-35” East longitude. The town has an area of 31.98 square kilometers but a large area of the town is underdeveloped due to severe topography characterized by high peaks, deep gorges and narrow altitude of Tuensang town ranges from 900 meters to 1371.60 meters. The town is perched on a ridge with general slope towards the Northeast direction and the slopes range from 40 degrees to 80 degrees. Three brooks, namely Yungyang, Lying and Tuensang Yung, split the ridge on which the town is established. The town has number of streams and rivulets flowing towards the valley from both sides of the ridge. The average annual rainfall recorded for the town is 200 cm (80”).
Tuensang is endowed with rich natural resources such as forest area providing environmental services. The soil is acidic, rich in organic, carbon but has poor potash and phosphates contents.
1.5.1.2. Shamator
Shamator is home to the Yimchunger tribe. This is one of the oldest sub-divisions which later got upgraded to ADC (Additional Deputy Commissioner) HQ; the land was donated by the Shamator villagers. It comprises of 11 villages, which spreads across the Saramati Peak and has very wide area coverage. The town was established on 1st January 1955. It has an area of approximately 15 sq miles. The town borders with Panso (Khiamniungan) in the North, on it south lay Kiphire district, on its west lies Chessore (Yimchunger sub-division) and on the east Thonoknyn (Khiamniungan). It is situated at 1818 meters above sea level. The town has number of important rivers such as Zingki and Yahee rivers. According to 2001 census there are 3400 population in Shamator. Agriculture is the mainstay of the people of this region; they practice Jhum (Slash and burn methods) and wet terrace or settled agriculture in some areas. The main crops of the region are maize, millets, Rice and variety of beans. Literacy is very low as it is all over Tuensang District.
1.5.1.3. Noklak
Khiamniungan are one of the major tribes inhabiting the eastern corner under Tuensang district in Nagaland having an area of 928 square kilometers approximately. This tribe consists of 28 villages with a population of 82,672 according to 1991 census are on Indian territory and the remaining 150 odd villages in Myanmar (Burma) occupying up to Khamti (Chindwin). There are two Government representatives and one Additional District Collector at Noklak and E.A.C HQs at Panso, Thonoknyu and Nokhu towns.
Khiamniungan tribal territory is bound by Myanmar in the east and west by Chang and Konyak in the north and Yimchunger in the South. The topography is severe, high hill ranges, which break into a wide chaos of spurs, ridge, and ranges. Each area has its own distinctive language and cultural features.
These people practice chiefly Jhum (slash and burn) cultivation, which occupies 871 of the working force. Besides this some of them engage themselves in weaving, blacksmithing and handicrafts to meet their daily requirements. Yet most of them face hard time due to crop failure which has serious financial implications.
1.5.1.4. Longleng (New District HQ)
Longleng is inhabited by the Phom tribe. Longleng, the tenth district headquarter of Nagaland is situated at an altitude of 1066.30 meters above the sea level with a population of 28,304 according to the 2001 census. The total population of the district stands at 118,905. It comprises of 26 villages, 2 EAC headquarters and 1 SDO headquarter under its jurisdiction. The District has an area of 885 square kilometers of fertile land and has vast potential for horticulture and agriculture.
1.5.1.5. Kiphirie (New District HQ)
The Saramati range, which has the highest peak in Nagaland at 3837 m. above sea level, is located at Pungro sub-division in Kiphire area. The district has a population of more than 100,000 living in 74 different villages and is also home to one of the only remaining rain forests in the region and inhabited by Yimchunger, Sumi, and Sangtam tribes.
1.5.2 Political environment

1.5.2.1. Population statistics
Tuensang district is inhabited entirely by tribes belonging to the Sino-Burmese group, which is the offshoot of the greater Sino-Tibetan groups. The total population according to the 2001 census along with the Kiphire and Tuensang districts stands at 414,801. The rural population of the district is 385,147 (93%) and the urban population of the district comprises is 29,654 (7%) only. However the provisional census data excluding the newly formed Longleng and Kiphire districts sub-divisions are stated here for reference in which the Tuensang district as of now stands at a total population of 1,89,791 people and 30318 households with 11 subdivisions and circles.
Longleng was inaugurated as a district on 26th January and the total census population of the town stands at 28,304 (2001 census) with male 14004 and female 14300 population (as quoted by Helper Samaritans) though Longleng as a district comprises of 118,905 population. The chief minister in his inaugural stated that “up-gradation of Longleng Sub-division to the status will generate and open new avenues and create wider opportunities….” and that “the people of Longleng deserve equal treatment.”
The Kiphire district has 106,105 population according to 2001 census and 17,357 households with 7 circles inclusive of the Kiphire Sadar, which was inaugurated on 24th January 2004. During his inaugural speech the Chief Minister stressed, “The inauguration of Kiphire district is the beginning of a new dawn and a new era for more than a 100,000 population living in 74 different villages…. and he assured the people of the new district that the government would do everything possible to bring …at par with other districts of the state….”
1.5.2.2. Traditional Governance
In Nagaland Tribal village councils regulates the social life. The regulation of 1945 gives powers of the Tribal Councils to try criminal and civil cases and to impose fines. They have the authority as long as the parties belong to the same tract all civil laws are tried by the council. Punishments are imposed according to the tribal customary laws although restrictions are imposed to restrict heavy or capital punishments.
The tribal land and customary rights are protected by article 371 (A) of the constitution of India. Special provision made in the constitution of India by means of the Thirteenth Amendment in 1962 inserted article 371(B) which provided (i) Protection of religious and social rights of the Nagas, Naga customary law and procedure, practices of civil and criminal justice according to Naga customary law and the natural resources. (ii). Governor’s special responsibility with regard to law and order in the state to be discharged in his individual judgment and for proper utilization of central grant. (iii). Special care for the Tuensang Division.
The 4th point Hydari Agreement, 1947 provides for non alienation of land belonging to Nagas to any non-naga .It also includes, The Naga Hills Jhum Regulation 1946, adopted from Chin Hills Regulation which safe guards and regulates the rights of indigenous people to Jhum land. Though there has been inclusion of Naga (Requisition Acquisition) Act 1965 and Naga Forest Act 1968, which provides absolute right to crave out forest reserves has given rise to controversial issues of protecting tribal lands which is unalienable. The backdrop provided briefly will help us understand that all issues pertaining to land, natural resources, and conflicts that continues to be settled within the parameters of the Naga Tribal customary practices.
1.5.2.3. Militancy and Peace
The Naga society has for long suffered unrest and separatist demands by armed militant groups who are powerful enough to control every walk of life. The presence of heavy military forces all over this border state has added to the troubles.
Recent peace efforts and a ceasefire between the armed forces and underground groups have provided a ray of hope. The people turned out in large numbers to participate in a peaceful parliamentary election in the state recently. The people hope that the peace process will continue.
1.5.3 Economic Environment
Ethnic and geographical isolation is one of the main problems that continue to contribute to increase of HIV/cases in the district. Two decades of prevalence of HIV/AIDS in the district without concerted efforts except for pockets of efforts from faith communities has increased the problems. Close proximity with one of the leading producers of Heroin no.4 in the world continues to threaten the youth and young children who are increasingly recruited to the addiction and ultimately the trade as peddlers. The older people who are addicted set bad examples too.
Economic deprivation is one of the main reasons that continue to lure young and old in the business of peddling drugs. Moreover due to marginalization even within tribes in the region as “backward tribes”, low literacy, inter-tribal clashes lead to regression in developmental activities have silently contributed to the siege of the disease and localized it. Poor educational facilities and lackadaisical attitude of teachers in the remote outstations continues to promote youth inadequate to face challenges and risk factors found in the environment. Thus also contributing to lack of employment opportunities, low status and high illiteracy of women, lost traditional work ethic continue to deepen poverty. Abject poverty due to tribal clashes, insurgency and factional fights is seen in some remote outstations of the district.
Bad roads, erratic electricity and poor communication facilities have plagued the entire district for long and people in larger settlements like Tuensang town feel harassed by the lack of basic facilities. Fortunately water available from natural sources in these mountains is of excellent quality though the efforts to transport water are literally back-breaking.
Deplorable road continues to be a major set back for local communities who depend on adverse climatic conditions for subsistence agriculture without or very few avenues for alternative income for sustenance.
Agriculture is the mainstay of the people of the Tuensang, Longleng and the Kiphire districts. According to the 2001 census, the 93% of the rural population 385,147 are rural and rural economy is dependent on the agriculture. Besides agriculture, the people of the districts are engaged in Black smithy, handicrafts, weaving, pottery, basket-making etc. The estimated cultivators and agricultural laborers comprise of 185,209 persons according to the 2001 census. The distribution of workers according to workers engaged in household industries was 1,562 and other workers category totaled 24,990 persons. Out of total of 414,801 population the census depicted that 229,592 were regarded as non-workers. Tuensang district comprised of a total of 157,760 main workers, marginal workers comprised of 27,449. The statistics thus provide a grim reality of the district of Tuensang, which in Nagaland considered as one of the main backward areas. Recipient to various backward development funds and border area development fund the district is yet unable to address the abject poverty that rages across large sections of tribal communities.
Cordial border trade relationships continue to exist among the towns and villages across the border between the Burmese Nagas and the Nagas inhabiting the Indian side. The International trade center exists at Pangsa under the Noklak block is in Tuensang district. There continues to be influx of Khiamniungan student community who come to Indian side for education and labor purposes simultaneously engaging in household services and receiving education.
1.5.4 Social & Cultural Environment
1.5.4.1. Chang
Chang tribe occupies the northern eastern part of Nagaland. As no written exist, legends in the oral form carry weight to the migration and origin of the nomadic tribe. Chang people migrated from the East in wooden canoes along the river Langyong and advanced westward on land. Thus the etymology of the name Chang is derived from the word ‘Chang’, meaning ‘East’. Another legend and traditional songs attribute that the Chang emerged from a place known as “CHANGSANGMONGKO” and settled at a place called “CHANGSANG” and this was the first named village of the Chang.”

A Chang Shawl
Traditional Social practices:
The Morung played an important role in the ancient Chang tribal society. It was used as a dormitory for unmarried men, who were trained, disciplined and learnt about adulthood. The older folk would narrate oral traditions passed through the ages, narrate cultural and traditions observed by the forefathers and acts of bravery and thus the Morung played a significant part in passing the age old culture, norms, practices to the younger generations. The place was also used for guarding and protecting the village from the attacks of the enemy.
Mr. Yamong Chang, Head man of Tuensang Village, 115 years old and still doing well.
The Chang like all the other Naga tribes were animist. They worshipped natural forces and were in awe of them, such as sun, moon, strong winds, heavy rains, trees, stones, hills and streams. Spirit of the forefathers were worshipped during troubled times. Ancestor spirit was believed to have influence on crops and general prosperity of their descendants. Other traditions associated with illness were observed, medicine men, tribal priest were called to appease the god of evil which caused illness by offering fowls or pigs. Traditional believed and observed the release of the scapegoat or a chicken which was released after going round the patient six times if a female and 5 times if a male after which the patient would spit on the sacrifice taking the illness and the curse of the sick persons.
Festivals:
The Chang observes six major festivals in a year, out of which three festivals namely, NAKNYULUM, KUNDANGLUM and POANGLUM are the most important festivals.
1.5.4.2. Khiamniungan
According to the mythological belief, the early ancestors is said to have emerged from a “Hole” in a place called KHIAMNIUNGAN, meaning, “Source of great waters.” The socio-cultural traits and religious beliefs of the Khiamniungan are same indicating one cultural identity and one language of both inhabiting the Indian and the Myanmar side. Historically the Khiamniungan were referred to as “Kalyu Kanyu” mentioned in the works of the anthropologists (courtesy-Furer Haimendorf).

Social practices:
The ‘Pou’ as morung is known in Khiamniungan had great significance in the traditional village life. It served as the center for social interaction and institution for handing down traditions, conventions and beliefs of the older generation to the younger ones. At ‘Pou’ young men learn social responsibilities of adulthood. It was a raised platform a place for gathering for meetings and drinking traditionally brewed rice beer. An important place where elders undertook decisions relating to welfare and warfare. Marriage was instituted between two major clans the Lam and the Shiu clans. Going against the societal norm is an offence, the defaulters considered as social outcasts.

A Khiamniungan shawl
Festivals:
The Khiamniungan observes various festivals with much fervor. Apart from MIU and TSUKUM they also observe festivals like BEI-AM, KHAOTSAOSE, LUAPLO, etc. Interestingly, most of the festivals are related to sowing of seeds and harvesting.
1.5.4.3. Yimchunger
According to the tribe they believe that the Yimchunger migrated from Burma and first settled in a village called ‘Kimiphu’ and later migrated to Yanger and then to Langa and to the present Yimchunger villages. The tribes live in two districts and Kiphire.

Yimchunger girls
Social Life:
Morung known as “Khiangyam” occupied an important place in the Yimchunger tribal society. A place for learning to be imparted, important decisions were taken and also served as a place for celebration during war victory. Yimchunger worshipped nature and gave due importance to natural phenomenon. They buried their dead under the bed of the deceased man. Marriages were fixed during the annual festivals

A Yimchunger shawl
Festivals:
The main festivals of the Yimchunger are METUM NEO, TSUNGKAM NEO, ZHITHSUT NEO and YUNTHSU NEO. Out of these festivals, METUM NEO is considered the most important. METUM NEO, literally means ME (SOUL) TUM (WRAP) NEO (FEAST). It is celebrated for 6 days from 7th to 12th August.
1.5.4.4. Sangtam
Sangtam tribe is one of the major tribes of Nagaland comprising of approximately 91,116 according to 2001 census. As true of different tribes of Nagaland the tribe has no written record of its origin though myths and legends have been passed down in oral form.

Sangtam youth performing a tribal dance
Social system: The Sangtam practice the hereditary chieftainship system known as the “YANGTHSARÜ”. The Chief of the villager is named as “OONG”. The law is maintained through the village court named as “Yukha Ku”. The court of “Yukha Ku” is composed of representatives from each clan. The clans were Throngru, Anaru, Jingrü, Mongzaru, Langthithongru and Rutithongru and marriage was instituted between the clans.

A west Sangtam shawl
Like all Naga tribes the Sangtam too practice animism before the advent of Christianity. To them, “all nature was alive with unforeseen uniform force”. The village priest called “Beruru”, magicians (amongru) and the medicine man was the very part of the socio- religious life of the tribe.
Festivals
The Sangtam tribe has about 12 festivals spreading over the calendar year including some special functions. All the festivals are concerned with the food production, blessings and prosperity. Out of the many festivals AMONGMONG is one of the most important festivals. It is the worship of “God of house and the three oven stones in the fire place”. The festival is observed in the first week of September every year.
1.5.4.5. Phom
According to the existing oral tradition, the ancestors of the Phom are believed to have originated from a place called Pongngaihong. They migrated from there to a place called Apaihong and later the ancestors migrated to Yingnyushang, the present place of the Phom. The mount Yingnyushang is considered the seat of all socio-cultural, political and religious practices.

Among the Phom the old tattooed headhunters are still held in high esteem
Social system:
As in the case of other tribes the Morung called “Bang” in Phom language was an agency fro all round social development. The place was a seat of learning and interaction among young people. Morung was a place where human skulls were hung during war as an acclaimed booty.

A Phom shawl
Festivals:
The traditional festivals of the PHOM are MONYU, MOHA, PANGMO, PONGVUM MO, HEHU MO and MAN MO while MONYU and MOHA are the only two festival celebrated with due importance.
- 1.5.4.6. Sumi

Sumi youth watching the fields
Sumi have two different clan-heads, viz. Swu (Sumi) and Tuku (Tukumi). By virtue of two separate clans the gennas and rituals differs between Sumi and Tukumi. Among all other festivals and gennas, Sumi in general accept the festival of Tuluni as the most grand and important one.
1.5.4.7 Log drums
Log Drum was the main instrument of communication among the Naga Tribes. The Chang called the log drum as “Tongsen”, while the Phom called it the “Shem,” the Khiamniungan called it “Phi”, the Sangtam called it “Singkong”.
The Drum conveyed messages or beats for war, beat of victory, festivals, during natural calamity or phenomenon such as occurrences of Solar and lunar eclipses. The object occupied the position of demigod in the village.
During the advent of Christianity into the Naga tribal communities the first destruction of Naga artifact happened to be the log drums. Even today these drums can be seen in each khel-sector of the clans.
Most Nagas follow the Christian faith mostly through their own tribal Baptist churches. Each tribe has its own church and services in their own languages. The traditional beliefs and practices though dwindling and discouraged by modern Christian faith, have not disappeared and are practiced in many pockets. Some ancient practices that Christianity has managed to abolish almost completely include head hunting and killing humans.
1.5.5 Health & Medicine
Tuensang district encompass the largest area and population in the state and yet has among the least health and medical infrastructure. According to the statistical record of Nagaland 2001 Tuensang remains fourth of 7 districts with 100 beds urban hospital and 50 bedded rural hospitals, 90 CHC, 96’s PHC, and 32 SHC, no Mental hospitals, nor T.B hospitals with beds. The Total number of patients treated in the year 2000, indoor as well as outdoor was 74,100 according to the 2001 census. While Kohima district has 30 specialists, Tuensang has no official specialist and 28 Assistant Surgeon 1 against 62 Asst. specialists in Kohima. The huge discrepancies in providing medical services continue to remain unresolved. Today Kohima has a total of 107 doctors while Tuensang continues to have 38 official posts with nearly 75% of absentees attached to Kohima and Dimapur hospitals.
Interestingly the vital rates of the district by Directorate of Economics and Statistics shows decline of infant death ratio since 1996 which had a record high of 29.13% in 1996 with a steady decline till 1998 with 6.82% and morbid ratio since then at 8.68% per thousand live births.
The interaction with various communities in the Longleng, Kiphire, Noklak, Shamator and Tuensang, presented a diverse findings and facts are presented here.
Longleng
In Longleng, the findings presented that 1 Community Health Center with 30 bedded hospital was upgraded 3 years back but there exists minimum facility with only 5 number of HCP including 1 MO., 2 nurses and 2 ANM. There was 1 sub center in Longleng, 1 in Sakshi area, 2sub-centers and 1 PHC in Yonga area, 1 dispensary and 1 PHC in Tamlu area. The district also has a temporary hospital ward for Leprosy patients with 20 beds but no doctor is available at the station and according to the information has never ever visited the site. There exists minimum Lab service for routine blood examination but according to the MO, the technician was frequently out of station.
The Medical officer has been in the station for about 15 years and in all his stay other doctors posted resided on only temporary basis. The hospital not only had inadequate infrastructure but did not even have enough space for expansion for infrastructure be it the hospital or for staff residence. There was no medical equipments, no lab equipments, only one trained technician, not enough medical attendants, no blood bank, no refrigerator for storing medicines nor blood products, No VCTC facilities whatsoever even to detect symptomatic cases even for clinical manifestation presented in the patients. The hospital has no proper water supply connection, as the pipeline remains without maintenance. Due to shortage of power supply, no generator the data are maintained either manually or not maintained at all in some cases. Inadequate staff and having to follow OPD procedure, they often did not have time to even register patients.
Tuensang town
There is one District Civil Hospital in Tuensang Town and the health facility comprises of 100 beds. Under the Tuensang District there is 1 rural hospital with 50 beds, 3 Community Health centers with 90 beds, 11 Primary Health centers with 96 beds, 5 Sub-Health Centers with 32 beds, 61 Sub Centers, 1 STD Clinic based at Civil Hospital Tuensang, 1 District Tuberculosis Center, 1 Post mortem Center The District as a whole has officially 38 Doctors, 99 Compounders, 166 Nurses. The District Civil Hospital provides basic facilities such as, 6 wards for treating –in- patients, STD clinic, PPTCT, VCTC, Regional Diagnostic under construction, Blood bank, with no proper utility, due to inadequate facilities Immunization programme for infants and children, General laboratory and DTC/RNTCP. The Health Care system is currently under the Medical Superintendent, 14 doctors but presently only 8 doctors avail their service at the hospital. There are 70 nurses including GNM and ANMS.
Kiphire Town
The Community Health Center of Kiphire District is a 50-bedded hospital but. But according to secondary sources most of the hospital furniture’s are broken. Due to shortage of manpower they do not maintain a separate STD clinic. Though there is a microscopic center for Sputum examination for clinical diagnosis for T.B At present there is only 1 medical Officer, though officially 3 should be posted at the CHC. There are 48 staffs. As most of the officials are out of station, access to primary care is almost absent in Kiphire with only 1 Medical officer, the patients are often treated with First Aid, they are unable to deal with terminal illness and serious cases due lack of proper medicines and basic amenities. Most patients are referred to Tuensang and Kohima hospitals.
Shamator Town
The Primary Health center is a 10 bedded hospital with currently 1 Doctor and 2 Nurses. There are 41 number of Health Care providers. Basic amenities are lacking in the PHC. The major health problems faced by the community in the assessed area are such as T.B, malaria, Diarrhea, Dysentery, Respiratory infection, kidney, UTI and STD cases.
Noklak Town
In Noklak the Community Health Center is 30 bedded with 2 doctors including the Medical officer and HCP 46 staffs. The major health problems faced by the community Such as Respiratory tract infection, T.B, STD cases and HIV/AIDS cases. There is a Microscopic center for sputum examination for clinical diagnosis for T.B.
- 2. HIV/AIDS Situation in Tuensang
The above statistics indicates rapid spread of infection among various groups – both high risk (as IDU, truckers, migrants) and non-risk yet vulnerable groups (ANC attendees, housewives).
The prevalence data for Tuensang from Sentinel Surveillance indicate much higher prevalence among both high risk IDU and pregnant women attending the sentinel ANC site.
HIV/ AIDS Fact Sheet - Nagaland
- According to NACO number of AIDS cases in Nagaland tripled from 103 in March 2001 to 343 in August 2003
Adapted from various sources (– NACO/ Gates/ NSACS)
2.1 Risk Behavior
2.1.1 Injecting Drug Use
The Voluntary Testing reports indicate high prevalence of HIV among the IDU in 2003 where out of 149 engaged in drug use - either in the past or those injecting drugs currently, 37 (25%) were found to be positive. The State Sentinel Surveillance for HIV infection among IDU population in Nagaland indicates high prevalence, with 47 (24.8%) IDU out of 189 tested positive. The injecting pattern adopted by drugs users often involved sharing of drug injecting equipment among the users. Cleaning needles before the other friend uses though common, the methods employed such as using water without proper sterilization is a leading cause of the spread of HIV/AIDS.
Diagram 1

The chart above shows that 25% of IDU tested positive in 2003 at VCTC.
Diagram 2

Awareness does not necessarily mean behavior change nor can the general populace be unaffected by HIV/ AIDS. Retreating behind a false sense of security assuming that only drug users or sexually active people are like likely to be infected is also a myth. No one is completely free from the ravages of this silent menace. However, in this state and especially in Tuensang a strong denial factor as well as refusal and failure to comprehend the intricacies and intensity of the problem is slowly destroying life, breaking families and relationships as well as the very fabric of the society.
The findings indicate that a majority of the IDU (present as well as ex-users in the high risk groups) admitted to taking drugs in groups and sharing needles despite being aware of infected needles being one of the modes of HIV/AIDS transmission. Once the drug starts taking effect (kick) the issue of HIV/AIDS becomes secondary.
Diagram 3

Diagrams 2 and 3 illustrate the Prevalence of HIV in Nagaland in the years 2003 and 2004. It is observed from the data that the percentage of IDU in the state is almost the same over a one year period – around 45 percent of the HIV infected persons are IDU. This is indicative of the high incidence of IDU behavior in Nagaland.
“We draw our blood, mix it with another users’ blood and if it is not sufficient, grind the tablets, mix it with the blood, then inject it…”
- An Intravenous Drug User recovering at Longleng.
Diagram – 4

Diagram – 5

From the data presented in Diagrams 4 and 5, it is observed that the HIV prevalence among IDU could have more than doubled over the last year. While in 2003, only 9 percent of all IDU were reportedly infected with HIV, between January and May 2004, 23 percent of IDU reportedly had HIV infection. This is alarming and indicates increased risk behavior related to injecting drugs.
Diagram – 6

Diagram – 7

In the above given Diagrams 6 and 7, the age range of HIV positive IDU has been compared between this and the previous year. The data reveals that in the year 2003, almost half the percentage of all HIV positive IDU (45 percent) were only 25 to 29 years of age, 30 percent of the IDU were in the 30 to 34 years age group and 14 percent in the 20 to 24 age group. However, the trend has changed over the past year with a vast majority of HIV positive IDU (71 percent) being in the 30 to 35 age group and the remaining 29 percent aged 25 to 29 years. This indicates possibly that more and more elder people are getting addicted to drugs (or getting tested) in the region than younger ones.
The behavioral determinants of the epidemic strongly pointed to a regular pattern of drug use in the local communities in all the assessment areas.
Respondents have mentioned difficulty in finding veins after constant drug use and so they help each other in finding the vein, a fact that increases risk.
When the supply of drugs is more and there is shortage of needles.
Intravenous Drug Use takes lesser time to get a ‘high’. Respondents reportedly undertake the habit to hide from family members injecting with the (same) syringe that takes lesser time but enhances risk of infection.
Economic factor- one does not have sufficient money to sustain the habit (individually), and hence is forced to join in groups and continue the habit.
“More fun to take it in a group-also the kick seems to be better when we take in a group”
It has been stated that a person who having adequate supply of drugs shares the same with friends/ other addicts so that whenever he runs out of stock, his friends (with whom he had shared) can come to his rescue and provide him with the drugs.
Respondents reportedly have fear of timely aid in case of an overdose.
The study has also revealed that there are cases when an infected person had shared syringes just to infect the other person out of anger and resentment for having discovered themselves HIV positive.
Another risk factor was the finding of injecting drug habit in one of the research area among users. Compared to other places in Tuensang, the level of awareness on needle sharing is much higher among the IDU in Tuensang Town and reportedly less common compared to others places (rural areas) in Tuensang.
Syringes and needles are also more easily available in Tuensang Town. However in other smaller towns, used syringes thrown by pharmacies are commonly used by IDU for injecting drugs. Awareness about safe syringes is also low among some communities (tribes). It has been reported by non-drug users that entire families share the same syringes.
Addiction to the drug prevents a person from taking any preventive measures. There have been many instances when the pharmacist was unwilling to give used syringes but the user did not leave the place unless he relents/ or simply picked it up from a garbage bin. They request pharmacists “not to throw it away.” This trend was present in Tuensang before intensive targeted interventions began in full swing.
“Initially we inject it in the veins (arms), then when we find it difficult to find veins in the arms we move on to veins in the legs then on to the arteries”
“Why should I be the only one to be infected, let others also get infected, we’ll all die together”.
(A strong feeling of revenge against society)
According to a survey by an NGO on the number of drug users in the main town in Longleng town between January 2004 and March 2004, they had identified 169 IDU and made 33 contact clients. The new district is reeling under the impact of drug use; the users gather in groups and wait at certain spots for the supplier/ drug peddler or the middleman to come with the supply. The numbers of users are so vast that they have an internal support system to deal with cases of overdose among themselves, hence, whenever such situation arises instead of bringing it to the notice of the qualified health practitioners they usually try to revive the person with saline water and often succeed in their attempt to do so.
In one community every evening users gather in large numbers near a stream and after having their required dose dangle their feet in the water tanks from where almost the entire community gets its water supply. Many of the users of this particular group also suffer from abscess.
During the course of this study, it was found that IDU (especially those who are bedridden) have a problem accessing good health care as transport facilities are poor and area is remote with inhospitable climate and bad terrain. The problems are compounded during winter months when some parts of Tuensang and neighboring districts remain snowcapped throughout winter.
The Drug trade
Myanmar villages and other border villages that are neither recognized by India nor Myanmar are said to be sources / routes of opium and heroin into the region.
The tribal communities that span the borders and live on both sides however strongly object to being branded as drug traders. A number of interests are likely to be involved in the drug trade and these are likely to include international crime and political players besides powerful traders.
Heroin is not the only drug that is abused and injected by IDU. A good supply of branded pharmaceutical drugs manufactured in India command a very high price in the illegal markets of Nagaland. These include spasmo-Proxyvon, other drugs and even cough syrups. Some of these drugs are diluted and injected by IDU.
There is a view among some stakeholders that lifting of prohibition on alcohol could reduce the demand for more harmful intoxicants like injecting drugs. The Mothers associations and some Faith Based Organizations object strongly to this view.
2.1.2. Multi-partner Sex
The study brought out a paradoxical scenario among drug users in relation to sexual behavior. While some alleged that sex ceased to become important once the drug began to take effect, others had a rather diametrically opposite view on the subject The latter group was of the opinion that awareness about HIV/AIDS became secondary once a person reached a ‘high’ on drugs. Alcohol supplied by the Army as well as the local bootleggers contributed to the problem. Not only unemployed youth but also others also indulged in high-risk activities after consuming alcohol and drugs.
Diagram – 8
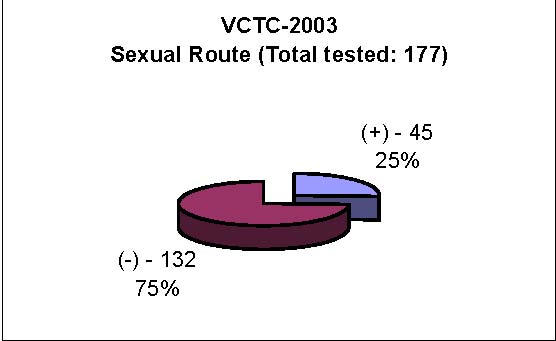
Diagram – 9

An analysis of the data in Diagrams 8 and 9 indicates that of the total number of cases who attended VCTC clinics, and reported multi-partner sexual behavior in 2003, 23 percent were infected with HIV. Comparatively, in 2004, there is an increase in the percentage of persons infected with HIV through the sexual route to 28 percent. This is indicative of the fact that sexual mode of infection is also prevalent among the IDU in the district.
This scenario can again be linked to the lack of recreational activities, pointing at the lackadaisical attitude of the Government toward youth welfare. The few schemes and loans facilities available for the unemployed youth are accessible only to those with high level contacts (with politicians and policy makers). Hence, the only option left for the unemployed/ frustrated population (which includes the educated as well as the uneducated) is to take to substance abuse.
Permissiveness observed through certain cultural sanctions among certain communities has led to youth even today taking to casual sex (without safe sex behavior) thus enhancing risk of infection due to multi-partner sex.
An interesting aspect about permissiveness in one particular community was observed is they had linked the issues of promiscuity of the locals with the inaugural ceremony of the town where a goat was sacrificed in the process. Since the goat is perceived to be a sexually active animal, the sexual habits of the people are thus believed to be similar to that of the sexual behavior of the goat that was sacrificed. If a different animal had been sacrificed, they believe that the sexual promiscuity would be lesser. Thus, socio-cultural myths and beliefs still continue to affect tribal culture effecting individual behavior and changes with respect to their family and larger society.
“Earlier a man could just enter a woman’s house and have sex without the parents protesting against the act. When the girl gets pregnant, the new born baby is wrapped in a cane basket (Khang), and left in the jungle”.“It is in the blood”.
This practice of free sex is still followed now as reported by respondents in Tuensang.
Diagram – 10

Diagram – 11
 A number of respondents accentuated that many youth actively engage in sexual activities (some reporting having sex at 10 yrs of age) and the parents admitted that they are not able to control the youth. Having multiple sexual partners is common and acceptable social behavior among many communities. Government officials reported that where young people hang out regularly in the evenings they have found many used condoms. Extra marital affairs as well as early marriages are a common feature among many tribes in Tuensang, Longleng and Kip hire Districts. There was reportedly a case where “…a young woman had kept track of more than 200 different sexual partners…”
A number of respondents accentuated that many youth actively engage in sexual activities (some reporting having sex at 10 yrs of age) and the parents admitted that they are not able to control the youth. Having multiple sexual partners is common and acceptable social behavior among many communities. Government officials reported that where young people hang out regularly in the evenings they have found many used condoms. Extra marital affairs as well as early marriages are a common feature among many tribes in Tuensang, Longleng and Kip hire Districts. There was reportedly a case where “…a young woman had kept track of more than 200 different sexual partners…”
It may be interpreted from the data presented in Diagrams 10 and 11 that compared to the previous year the age range of percentage of persons infected with HIV is increasing to 25 years and above. This also compares with age data of IDU that indicates similar trends. It is thus established that multi-partner sexual activity is common and socially acceptable. Furthermore, increasing number of older respondents are getting infected. Many of the respondents also said that they do not insist on condoms if their partner is unwilling and many admits that once a person is high on drugs or alcohol, condom use is not accorded importance. PLHA interviewed also said that their partners do not want to acknowledge their positive status nor use any preventive measures. These indicate added risk and increased vulnerability among those likely to pass infections through sexual route.
The study also reveals that 14-35 yrs age group is more vulnerable to STI (Sexually Transmitted Infections). Interviews with the MO (Medical Officers) indicate that 5-6 cases are handled individually by the MO every month. One of the MO interviewed in one of our study area said that earlier there were hardly 5-6 cases in a year, but from 2002-2003 he has handled more than 40 STI cases. There is high prevalence of STI in some areas.
The findings of this study also show that majority of STI patients are from the general population. This excludes the number of people who try self- medication like Ampicillin as it dries up sores during the primary stage (Ulcers) and (they) approach the doctor only when infection reaches the secondary stage (Syphilis).
The study also brings out that people in the High Risk Category are usually IDU. The sexual partners of IDU who are both at risk of infecting them and getting infected include primarily significant partners, (including spouse) sexually active people/ wine brewers (consensual sex in Tuensang community) partners/ spouses of current and ex-users as well as antenatal cases.
A small percentage of the local population who also falls into high-risk group category are those married to the migrant community especially the Border Road Organizations who are stationed at different places at different times and who cohabit with the local community especially with the female population wherever they are stationed, increasing chances of transmission of HIV.
“Out of 100 patients who come for treatment, 20 percent are STI cases (mostly women-married as well as unmarried) and as many as 60 to 70 percent of deaths among high-risk groups are clinically diagnosed or suspected HIV/AIDS-related deaths”.
As quoted by a Medical Officer in the study area (Tuensang)
Case Study of clinically suspected HIV case
“One of my patients repeatedly complained of weight loss, dehydration, darker complexion, loss of stamina/ feels weak all the time. The patient could also not take alcohol or non-vegetarian food. Despite repeated treatment for OI(Opportunistic Infections), he was not responding. I even went to the extent of giving him DXN and other medicines out of my own pocket. I clinically diagnosed his status and sent him to RIMS (Regional Institute Of Medical Sciences), where he was found positive after the fourth test. He came back and revealed his status to me. I had to give him counseling, as we don’t have this facility here. Looking back at his case history I found out that he got infected in Imphal. His wife was found negative on the first test but since she is six months pregnant I’ve advised them to go for further testing”.
-Medical Officer in small town without testing facility. Only Tuensang town has a VCTC in the entire district
2.1.3 Parent to child Transmission
Diagram – 12

Diagram – 13
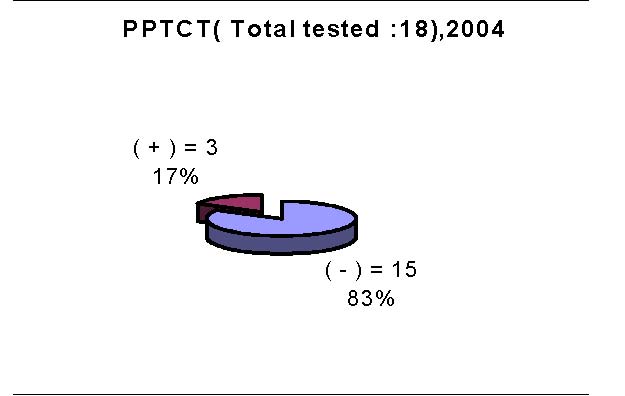
The PPTCT report from 2002 September indicated that out of 27 tested 5 (19 %) were found positive. The data from January to December 2003, Civil Hospital Tuensang, shows that out of 213 antenatal mothers given counseling, 97 went for testing out of which 5 (5%) were found positive. As illustrated in Diagrams 12 and 13 above, January 2004 to April 2004 report of PPTCT shows that out of 30 antenatal mothers given counseling, 18 were tested and 3 (17%) were found seropositive. With the exception of Tuensang Town Civil Hospital there is no access to VCTC and PPTCT in the other study areas. But various incidences were reported where both the spouses who were into substance abuse have passed away or repeated attempts to have a child have been a failure - reasons attributed to it were either more than one miscarriages or losing the child after delivery. There are also cases of conformed PLHA as well as suspected PLHA cases (reports from the medical practitioners) whose spouse is pregnant but have not gone for HIV/AIDS testing. The issue addressing PPTCT have not been addressed in three of our study areas.
Reasons for extremely low usage of condoms and inconsistency in use of condoms has been attributed to several factors that have strong roots and bearing on efficacy of condoms as an effective prevention tool. Its use is discouraged – especially among women as use of condoms is linked to issues of morality (lose character). Religious sentiments and the controversial stand of Christian institutions place restrictions on the use of harm reduction measures such as condoms (being an artificial means of birth control).
2.1.4 Blood safety
Though blood safety norms are present and regulations exist, it is to be seen whether such measures are being adopted scrupulously in the state. This pertains to transfusion of blood, precautions taken during delivery of infants (especially in the case of HIV infected women) and a monitoring of blood safety measures in the state. What is also critical is availability of safe blood during medical emergencies. Though Government institutions reportedly follow procedures and maintain stocks, the same can be said only of the main state capital Kohima or district headquarters hospitals – Tuensang and other main districts. Even in newly formed districts such as Kiphiri and Longleng, blood safety and availability are a far cry.
Private blood banks operate in the state but monitoring of the same is warranted to ensure quality services and at affordable rates making the same accessible to all who need it.
Another issue related to management of blood and related issues is its handling and transportation, issues pertaining to storing, and successful transfusion. The state is burdened with logistical problems with bad or no roads in remote inaccessible areas, frequent land slides and bad terrain, inhospitable climate, erratic power supply affecting medical emergencies, failed communications links and administrative bottlenecks.
What is needed is a strategy to identify barriers, prioritize problems and address them based on the community’s perception and thus overcome issues pertaining to blood handling and safety with emphasis on prevention of HIV transmission.
2.2 Impact of Risk behavior
Data obtained from VCTC/ PPTCT as well as information from various medical practitioners shows that mode of transmission through sexual route have been increasing though there is a sharp decline in IDU overdose cases in Tuensang Town, which again shows a contrasting differences with the other two new districts under our study area.
Data as well as various interviews with Medical Officers, counselors of VCTC/ PPTCT/ IDU/ PLHA during the course of the study shows that the mode of HIV/AIDS transmission is more through sexual route than through infected needles. Tuensang Civil Hospital VCTC report of 2003 shows that out of 432 counseled, 400 went for testing and 82 were found positive (32.8%). Between January 2004 and March 2004 VCTC report shows that out of 39 tested, 11 were found positive (42.8%).
Denial of HIV/AIDS by almost all sections of the society is one of the major factors spearheading infection. Moreover it is not uncommon to find not only the youth but also the middle aged in the community having multiple sexual partners. Many also knowingly indulged in risk behavior despite being aware of the other person’s sexually active life.
Interviews with the PLHA as well as secondary information received from MO (Medical Officers)/ counselors/ social workers reveals that almost all PLHA have not less than 5-10 sexual partners and all the PLHA interviewed by the team are either married or are having live-in partners.
One of the respondents (PLHA) said that she may have been infected by one of her partners who were an IDU. She has an infected womb after undergoing an abortion at home by injecting when she was two months pregnant. She has a chest problem and also under went TB treatment in Dimapur but could not continue the course due to financial constraints. She is also not satisfied with the facilities provided in the Civil Hospital Tuensang and feels discriminated whenever she goes for treatment. Two of her previous partners are now married now settled back home in the village.
One of the PLHA (tested positive in November 2003) having a live-in partner responded that he has not disclosed his status to his partner. He was on Brown Sugar for 6 years, was off drugs during 1992-93, and then started injecting SP; he also shared his syringes despite being aware of HIV/AIDS and attributed it to a psychological need. He also suspects some of his friends to be infected but says that they don’t want to accept reality, and many feel that they are “better off being unaware of their status”. He admits that though he wants to reveal his status to his partner, she does not want to acknowledge the existence of HIV/AIDS. He is also suffering from STI, despite repeated treatment for OI. It always relapses, as his partner is unwilling to come forward for treatment. Despite numerous visits by the counselor she has not responded positively. Most of the times both also refrain from using any preventive measures, and condoms given by the counselor are not used (they feel lazy to use it) or are usually given away to friends. When asked about his consent for agreeing to go for testing, he said that he hope to get access to medicines to prolong his life. His family and also his neighbors suspect that he is positive as he has lost a lot of weight and falls ill constantly, yet he has not got the desired support to be open about his status. He is also stigmatized by some of his neighbors. He has shared his fear of dying early.
2.3 Harm reduction
There is no visible needle exchange program in the district.
Condom survey findings show that condoms are rarely available in shops other than Pharmacies. Shops and Pharmacies are in any case open only for a few hours in daytime. By 4 pm most shops start closing even in Tuensang town. Purchase of condoms is done mostly by young people (mostly males). Many educated young hesitate to buy condoms from the pharmacy owing to taboo on such a practice. This indeed is a worrying trend when almost every section of the community has reportedly said that sexual activities are very much prevalent amongst the unmarried as well as the married population. Statistics obtained from medical department/ data from NGOs carrying out interventions indicate the spread HIV/AIDS through sexual route higher than that of infected needles/ syringes. Findings also show that risk behavior also leads to higher risk. However, there are many misconceptions about chance encounters and timing of infection. Many do not realize that for instance, a single encounter without safe sex practice can result in HIV infection.
2.4 Gender
Gender inequity is also an issue that needs to be addressed adequately. Societal norms are more tolerant and sympathetic to male drug users compared to female users.
The study also brings out that women fall in the ‘more vulnerable’ category than men. A high number of women in the high-risk category reportedly stated that their partners are not aware of condom use and are against its use. Some also mentioned that if a woman were to initiate condom use she is perceived to be promiscuous despite her partner’s drug habits or is suspected to have had/ has an active sexual past/ present life. Many women in the high-risk group (HRG) have also been infected because of their partner’s past/ present drug abuse habit compounded by their refusal to acknowledge that they might be HIV positive. Women Support Groups belonging to the high-risk groups hardly socialize with others. Even during this study, they appeared very apprehensive and not forthcoming with information on the HIV/AIDS scenario and its impact on people like them. A sense of fear seemed to grip the group, who showed signs of insecurity. The only group to address the issue of Orphan and Vulnerable Children (OVC) was the women’s HRG support group in Tuensang Town who said that the group members would take care of the children of positive people by providing the necessary moral, emotional, physical and financial support.
“I am HIV positive and feel extremely depressed when I think of my positive status as I know that there is no cure. I also know that I’m going to die of AIDS and it’s a frightening feeling - of dying without family and without community support”. - HIV Positive IDU who has disclosed his status openly, Tuensang
“If a person sleeps with a person who practices high risk behavior without taking any preventive measures, then the next time he becomes slack in his/ her attitude in taking any precautions thinking that he/ she is already infected by the previous encounter”.-Views stated by an ECS Support Group member at Tuensang.
2.5 Knowledge & Awareness
Majority of the respondents feel that the mode of transmission was more through drug use and unprotected sexual contact with an infected person, though many of the respondents had inhibitions to talk about the spread of HIV/AIDS through the sexual route. With the exception of the Medical Officers, all cross-sections of the society including those educated had but a basic knowledge on HIV/ AIDS and were confused, puzzled or ignorant about drug use and its relation to spread of STI/ HIV/ AIDS. A few did not even hear about HIV and AIDS. In one place though it was apparent that the entire community was confused they do not want to acknowledge the intensity of the problem. A general feeling among the elders of this community is that the youth in the age group of 14 to 25 years are more prone to getting infected by HIV (owing to increased risk behavior). Various groups have conflicting opinion about the route of HIV/AIDS transmission in their community. It is a classic case of passing the buck where the elders blame behavior of youth – consumption of alcohol (both locally brewed rice beer and Indian Made Foreign Liquor (IMFL) that is sold by bootleggers or exchanged by trading shawls with the army Assam Rifles regiment) leading to unsafe sexual practices enhances risk and HIV infection, while youth point at IDU for spread of HIV in society. The IDU on the other hand feel that the general public including elders are responsible for spread of HIV through the sexual route.
“There were a number of women users in our area but their rehabilitation was not addressed by any in the community. In sharp contrast while male ex-users were hailed as outstanding examples as agents of change in almost all section of the community, with the exception of one group, which commented about women luring men to addiction, drug use amongst womenfolk was not even acknowledged as a problem”.
Comments by women stakeholders in Longleng district
Non-involvement of the primary stakeholders –youth, community elders, women, health care providers, PLHA and influential ‘gatekeepers’ has resulted in creating several stumbling blocks in smooth launch of intervention programs. The ground situation reveals that the IEC programs on AIDS awareness conducted by District AIDS Control Committee (DACC) of Tuensang has undone more than achieved what it sought to among the target community as it seems to have left the general public in a state of confusion as well as with several misconceptions as many still viewed that harm reduction measures and activities such as open condom demonstrations indirectly encourage the youth enhancing their curiosity that might motivate them to experiment in sexual activities at an early age. This indicates that the sentiments of the Naga people and their open views on sexual freedom (permissiveness) have been either misinterpreted or have not been given due consideration.
Awareness on HIV/ AIDS among the general public is reportedly higher in Tuensang Town compared to other districts in the assessment area. Among some communities (tribes, especially those in far-flung areas) the level of awareness is very low. Some of the respondents in the qualitative assessments indicated that awareness levels on HIV/AIDS are as low as 5% in their community (though this can be corroborated only through scientific quantitative study or ‘triangulation’ of various methods. The fact however remains that awareness levels are pretty low and a high prevalence state with several high prevalence districts cannot afford to keep knowledge and awareness levels among persons facing epidemic proportions the way it is at present. They repeatedly mention that only the educated have knowledge about HIV/AIDS and are confined to urbanized areas.
In this particular community, outreach workers who intervene among HRG encouraging them to go for testing in order to access care and treatment facilities were labeled as “witches who hunt for blood” and also strongly felt that social workers should leave the drawing of blood samples to medical authorities. Due to this HIV/ AIDS has been termed “Donathou Khio” meaning “something that causes extinction”. Religious confirmation also strongly advocates and influences the mindset of the community. This is visible in the following sentiments expressed by one of the religious teachers during the assessment.
“With regard to knowledge and awareness on HIV/ AIDS, we can categorize three groups of people: First, those who are educated and understand about the HIV/ AIDS pandemic; Second, those who know about basics of HIV and AIDS but have no access to harm reduction measures such as condoms and syringes; and third, there are rural illiterate masses who have not heard about HIV/ AIDS at all”. - A key stakeholders during the qualitative assessment, Tuensang
Astonishingly, only a few respondents mentioned HIV/ AIDS transmission through blood and blood products. Many however admitted to the high numbers of drug uses in their community but did not acknowledge the prevalence of HIV/AIDS. Many also opined that (if ever there were reportedly persons with HIV/AIDS) they would invariably be only those who interacted with people of other communities.
A small section also said that HIV/AIDS is spread through lack of personal hygiene/ lack of sanitation. A few were under the misconception that sharing food or touching and kissing an infected person could spread it. Among members of two communities (hailing from Shamator and Noklak) in the assessment, they opined that using condoms was 100 percent safe while on the other hand were under the misconception that frequent use of condoms would make one vulnerable to many diseases.
Knowledge on mode of transmission from mother to child was very low among all sections studied. A few organizations were against harm reduction programs like condom promotion and needle exchange programs. They opined that these kinds of programs might bring down the HIV/AIDS ratio but in turn would promote/ induce curiosity about drug use and early initiation to sex life among the youth.
A section of the respondents particularly the youth responded that programs related to HIV/AIDS are just to discourage free sex or bring down sexual activities. Some held the view that HIV/AIDS programs were meant mainly for the IDU only because according to them elders in the community neither know about or have they seen condoms.
“We do suspect HIV/ AIDS incidence in our area but unless we see it visibly we cannot be assured of its existence”.
Comment by Teacher from Shamator reinforcing religious sentiments in relation to HIV/ AIDS
“An mysterious sickness and a classic disease, so the government should not concentrate on finding a cure but make the public aware, If the public is educated then people will accept the PLHA and people will not be embarrassed by this disease”.
Respondent’s feedback to current HIV/ AIDS knowledge scenario
“In olden times they (people) believed all sicknesses could be cured. “Scabies” it was considered, could be cured in three years and it was believed that STI could be cured within a period of six years”. “When someone was suspected to be infected with STI, news spread silently and such people were avoided for six years”. “Thus, HIV/AIDS also can be cured in this way” (taking prolonged cure and abstaining from ‘risk behavior’).
Views expressed by Tribal Leaders from Noklak.
2.6 Status of PLHA
Societal transformation based on human rights culture is an imperative need and this sensitization has to be there at the individual, family, community, and society level. Only through a sensitization process that recognized the inherent dignity and equal rights of all can human rights be realized. Fear becomes an undeniable and unavoidable factor when one comes to know about one’s positive status.
Disregard and contempt of one’s right to live with dignity intensifies the fear, it is an issue that needs to be seriously pondered.
Stigma and discrimination of PLHA is very much prevalent in all the areas. One major factor contributing to it is people’s refusal to accept that they are responsible and must do something to solve the problem. Baring a few, almost all sections of the community had extremely prejudiced views on HIV/AIDS.
Even those who wanted to address the drug problem had a biased approach. The most commonly heard refrains from almost every quarter was the situation is complex since users who show symptoms of HIV/AIDS do not want to acknowledge the reality of being infected actually infected by the killer disease.
For instance, in a sample community, it was analyzed from secondary data obtained that out of 90 IDU tested for HIV, 33 were found to be positive, out of which only 2 of them belonged to an outside community.
Solutions given to address the problem by different sections of the community in fact reflected stigmatized viewpoints. Some community’s criteria to help the infected person was that, the PLHA had to declare their status to all sections of the community, where as on the other hand they also said that almost all the users have died (only 20-30 users) so there won’t be any positive cases, they also said that they do not want false reports about HIV/AIDS in their community, in case there are cases, report should be given to the court.
Only a small section acknowledged and admitted that they fear that HIV/AIDS is very much prevalent in their community despite lack of medical evidence or without coming into contact with an infected person. The findings also presents paradoxical scenario in some intervention areas. The church wants to intervene and address the problem of HIV/AIDS. While some had a more moderate view on promotion of condoms despite setbacks “open demonstration of condoms by the church had more set backs as people did not like the church openly taking about it, but that does not mean that we don’t advocate it’s use to our infected clients” In Nagaland the Church is a powerful platform through which awareness as well as the issue of stigma and discrimination can be addressed. Yet there is also a lot of stigma and discrimination from the church leaders as they are still entangled with strong religious moral perspective and believes that there should be a separate Rehabilitation center for the +ve people and their needs should be met by the government and not the church or the community. Some Church leaders cited moral teachings where lepers were considered an outcast and suggested that PLHA should also be kept in the same manner.
In one community where ECS/ CACS (Churches Alliance for Community Support) is working they have even stopped distributing condoms to positive clients. Even on the issue of supply of syringes to the users they were of the opinion that they will allow it but not encourage it or find alternatives for disseminating information. This also raises the question of how the church is going to address this problem-of reaching out to the general populace - people who are not married and do not abuse substance, but are sexually active or are married to a HRG spouse. On the other hand despite sincere efforts by the church to address the HIV/AIDS issue, some sections of the community strongly protested against the Church advocating any preventive measures,
“We discuss this in the Council meeting and agreed that for Christian’s condom is not necessary, KBCA or Churches cannot promote condoms, it has to be done only by the medical department, the condom program is promoting sex only, and we want total abstinence”. Many were also of the opinion that teaching of God’s word would be more effective than promotion of condoms and syringes.
Except for women who were in the high-risk groups and some NGO’s of Longleng and DB’s of Kiphire the issues of affected people including OVC (Orphan And Vulnerable Children) was not taken into consideration by any section of the community. In fact many did not want to talk about it and dense denial of accessing care or support was not even recognized.
Views revolving around People Living With HIV/ AIDS (specifically IDU)
“When I first heard that I was positive I wanted to die, I felt people will discriminate me and my family will also forsake me” – (Interview with a PLHA).
“Remaining undisclosed about one’s status itself is a torture as deep down an infected person is longing for love, care and support, as well as fulfillment of one’s need”
(Survivor Support Group of Tuensang).
Attitudes and opinions varied from moralistic to judgmental to “I’ve seen it all and I know that there won’t be any changes” to a desperate plea for help “please help us to do something for the younger generation; we have lost all our young people to drugs”.
“We have a drug problem, but we don’t know about HIV/AIDS” / “HIV/AIDS does not exist in our community, if there are cases of HIV/AIDSit will only be among people who interact with people from another community”.
“We are afraid to tell them that they might be infected as we fear reprisal in the form of denial and anger” quote- MO in one of the research area.
“I am against HIV/AIDS programs and the result of high prevalence rate of HIV/AIDS cases in my community, it is not a fact, comparing to other areas, HIV/AIDS is very less in this area because IDU are very rare now as they have to know the outcome of injecting drugs”- quoted by a Government official in a community where testing facility is not available.
Some opined that the solution lies in letting positive people marry each other. “Dump them in the garbage bin or burn them”, “Take blood test sector wise of all suspected people”, “We won’t go near them”, “They are infecting the entire population” were some of the comments of this group despite promising manpower and also giving word that they shall see that the blood bank facilities are made available to the general public (Municipal Committee).
The finding also brings out that education as well as access to information can be a part of the solution if implemented sensitively but it cannot completely break the barrier when it comes to stigma and discrimination. Despite every group emphasizing on the importance of awareness programs/access to information among all sections of the society as well as targeted interventions programs among IDU as a solution in doing away with stigma and discrimination, in reality this has not been possible till date. There are glaring examples of the community not coming to the person’s aid despite being open cases including his/her immediate family members, as well as numerous incidences when a person has been stigmatized on mere suspicion.
Dense denial strongly also comes from people who have had access to statistical information. Some have even said that data given out by the government with reference to Tuensang district are “grossly exaggerated”, which in turn is giving out a very negative message about it’s people as people are starting to have misconceptions that “everyone who hails from Tuensang is suffering from AIDS”. Comments like “I feel that condemnation should be there. Interventions programs will only encourage drug use, when we stop catering to their needs (users), the future generation will see that and learn to keep away from it” or “shoot them, well! Sometimes I feel that it is better to just shoot them, which is the only way of stopping it”. “You are simply unlucky if you are a first time offender” came from educated people. Some Govt. officials as well as some NGO’s firmly stated that they will never give a job opportunity to a PLHA as it is a matter of compromising on the prestige and dignity of the organization.
Family prestige as well as clannish feeling becomes an issue when it comes to acceptance of PLHA within the family or community set up. Some opined that 75 percent of the community would not only discriminate the PLHA but also their families and the whole clan. Many parents who have lost their children to addiction or HIV/AIDS-related deaths are still denying the fact that they died due to AIDS. They felt disclosing their status would ostracize them and creating an enabling environment for them to disclose their activities will indirectly encourage more anti-social activities. All sections of the community have said that the present environment is not viable for the PLHA to disclose their status.
Some also expressed that it is the responsibility of the Government to take care of the infected people and not the community and felt that Health and Family Welfare Department would be the best body to address this issue. They also opined that there are many NGOs who have not implemented programs effectively.
2.7 Stigma & discrimination
A survey was conducted among 500 respondents from major churches such as the Chang, Sangtam, Yimchunger, Khiamniungan and Ao tribes to assess the issue related to stigma and discrimination.
Out of 491 respondent 384 (78%) of the informants were of the opinion that they were willing to share meal with the PLHA and only 84 (17%) responded that they would not share meals.
The query as to whether they would care for male relative who was infected, the majority of the respondents 424 (87%) responded that they would care, while 44 (9%) respondents were not willing to provide care.
Out of 485 respondents, 345 (71%) were of the opinion that they would buy food products from an infected shop-keeper, but 107 (22%) were not willing to purchase it from there.
When it came to family response towards HIV/AIDS person in the family, majority 235 (49%) out of 487 respondents wanted the status to remain a secret, and many 219 (45%) also responded that they would be open about the status.
The study also included a question as to whether the PLHA should inform the husband or wife and majority 440 (90%) were of the opinion that they should inform the spouse of their infection.
- 3. Current Responses to HIV/AIDS
The current responses to HIV/AIDS across Tuensang District have been described in this section.
3.1 Longleng
Cutting across all cross sections of the society in our research area, Longleng stands out as a community that identified the problem of drug-use in their community without any outside agency’s intervention but is still to come to grip to handle such a problem. In Longleng the Deputy Commissioner is spearheading the initiative of involving the whole community to address the issue of drug problem in their community. During this assessment, an appeal letter that would later be translated into the Phom dialect has been sent to all stakeholders in the community. According to the DC, “The issue of involving the entire community has been constantly crossing my mind. We should identify the drug users / HIV positive people. I feel the use of drugs should be arrested”. He also expressed that the community will have to find ways to minimize it/ stop further spread/ after identification gives them counseling/ interacts with them/ organizes youth camps instead of rehabilitation center/ share the word of God/ sees that they repent. “The Church should play a vital role in launching programs, enlist households, identify proper treatment, affectionately interact with them, we should also know their problems, grievances and frustrations” added Mr. C. K. Nikhekhu, DC of Longleng - the newly created district. “If the public approach me I am willing to give 100 percent departmental support to them”, said Mr. K. Walling the SDPO of Longleng. “We are ready to fully co-operate in every way”, remarked the Hukpang, Orangkong and Bhumnyu villagers (HOB) the original land donors of three villages that helped in the establishment of the Longleng Town. The Association of Phom Graduates and Officers of Longleng stated, “We are ready to provide all the resources locally available, all possible manpower, even land as well as extend help in every way”.
The Phomla Hoichen, which is the apex women body of the Phoms in collaboration with ECS, has officially agreed upon to take up interventions among drugs users and initiate women’s response towards HIV/AIDS care and support. The NGO is also presently advocating to NSACS (Nagaland State AIDS Control Society) for intervention facilities to be made available in their district. Testing facility is urgently needed in the new district as the community is faced with the huge drug addiction problem. The Phom Baptist Christian Association in Longleng commented “We feel a sense of hopelessness, rage and yet at the same time we also hope and pray for a change and we, as PBCA will render full cooperation”. The PBCA provides sizeable assistance to the community. A Drop-in- Center by Yingli Mission Society under the aegis of NSACS was inaugurated in March 2004. Helper Samaritan an NGO initiated by a MO of Longleng is doing a survey of identifying users in the community so that further intervention programs can be carried out in the community.
3.2 Kiphire
USSC (United Sangtam Student Committee) the apex student body of Kiphire has been networking with ECS intervention programs in their area. The student leaders of Kiphire also promised to fully co-operate in every way “We are willing to integrate HIV/AIDS programs in our activities, as well as sacrifice everything”- Student Leaders of Kiphire said. “We will fully co-operate, even donate land”, added GB’s Union of Kiphire who also opined that “We don’t have any information nor knowledge so we can’t even identify needs - all we know is that we have to address this issue. We also have to address mother-to-child infection. We will render all possible help to any organization who works here. If programs are implemented for care and support for infected people we will fully cooperate”. The Women Welfare Association & Working Women of Kiphire and International Border People Welfare organization. (NGO sponsored by NSACS) also voiced similar concerns, “We will help in every way if ECS intervenes in our community. We will collaborate and work on this issue”. Thus, tremendous amount of energy and interest is apparent in this district with every known institution willing to pitch in and play an important part in HIV/ AIDS care and support programs for among IDU.
3.3 Noklak
The Khiamniungan Baptist Association Targeted Intervention and CACS under ECS. Seeing the intensity of the needs, individuals are also coming forward to address the issue in their own capacity. “I’ve got myself involved in giving medicines for OI in collaboration with ECS/ CACS”, remarked a pharmacist of a local store.
3.4 Shamator
A DIC (drop in center) was opened under the aegis of ECS. Two volunteers are appointed by YBBA (Yimchunger Baptist Association) and two Support Groups have been formed among IDU’s in Shamator.
3.5 DACC- Tuensang
The District AIDS Control Committee of Tuensang is headed by the DC (Deputy Commissioner) who is responsible for undertaking IEC-related activities in all districts of Tuensang. Under the auspices of the Nagaland State AIDS Control Society, the district level AIDS committee has been formed in all 8 previously formed districts. With the collaboration of the NGOs in each district, the committee disseminates information in all peripheral areas. However, it is acknowledged that awareness levels are stil extremely low and hence there is need to multiply IEC dissemination through making use of appropriate channels and communication media to dispel ignorance and misconceptions around HIV/ AIDS among all stakeholders and the general public. Various Inter-School competitions on HIV/AIDS awareness are conducted by DACC and also conducts training for village-level stakeholders similar to that conducted among Urban dwellers on HIV/AIDS.
The DACC has over the last two years created village level health volunteers in over 200 villages in the district and has trained them in the basics of HIV/AIDS. These volunteers are being provided a monthly incentive to carry out outreach activities. The DACC is aware of Behaviour change Communication skills needed by the volunteers but do not have sources of technical support to provide such training.
3.6 ECS - Tuensang
“Rebuilding is a time-consuming and painful process but recovery is a reality”.
Members of ECS understand fully well the meaning of this maxim and are leaving no stone unturned to realize the project objectives as planned. Currently there is an added emphasis on adopting and integrating the GIPA principle, thereby empowering PLHA and bringing them into the mainstream with total community, family and professional support.
-
a. General community
Various workshops and seminars have been conducted among all cross sections of the community outside Tuensang town. The organization conducts stakeholders meetings at all the intervention spots covering Tuensang town, Shamator town, Noklak town, Longkhim town, Chare town, Thonoknyu town, Tobu under Mon districts, covering in all 24 villages and 112 hot spots.
Similarly, a seminar was conducted by ECS among various service providers, that led to the formation of the Tuensang Public Forum.
A joint venture has been attempted seeking to integrate HIV/AIDS programs into religious/ faith-based activities conducted by the community and custodians of particular faiths.
Information concerning HIV/AIDS programs/ statistics of the District has been shared with all the major stakeholders of the community within the districts and the state.
Inter-youth debates and seminars in sectors in the target villages and towns are being conducted with the theme on ‘Drug Abuse and how youth can be saved from such a social menace’.
b. ‘Catching them Early’ - School education
ECS initiated formation of Core Groups since 1996 among school children so that they can disseminate information to their peers. A peer educator leader is selected from each school. Poster/painting/quiz competitions are some of the activities undertaken under this program. A total 16 schools and 2 colleges are covered under the programme at present. ECS has trained more then 200 teachers as Counselors. Provides a board called “Express on Board”, to initiate students and teachers to provide information in schools. Sister schools had been adopted to nurture other students from other schools to participate in anti-drugs/alcohol/HIV/AIDS programmes. Painting, drawing competitions are held annually.
-
c. Advocacy efforts
Currently ECS is networking with Phomla Hoichen, an NGO (women’s group) for targeted intervention programs among drug users and HIV/ AIDS/ STI intervention in Longleng district.
Networking between ECS and Helper Samaritan an NGO in Longleng is being done that sends IDUs in batches to the rehabilitation center in Tuensang run under the aegis of the ECS.
ECS Networks with USSC (United Sangtam Student Committee) for implementing targeted intervention programs among IDUs in Kiphire.
d. ‘Prevention is better than no cure’ - IEC wing of ECS on a dissemination spree
Pamphlets, posters, bill boards, wall writings in English and in the local dialects are posted in all intervention towns, spots. The organizations prints tracts for IDU’s for “Safer Drug Use”, provides pamphlets on HIV/AIDS statistics.
Building relationships through Tuesday Fellowship (sector-wise) where the main focus is on both parents and IDU’s, and Friday Fellowship (NA groups meetings) in the ECS office premises particularly for the users forms an integral component of the participatory and trust building process of ECS.
e. Care Component Of ECS.
Churches Alliances for Community Support:
CACS under ECS care component is a network among the five major Churches of Tuensang, KBCA stationed at Noklak is to provide Care and Support to PLHA and their families.
The major Churches include:
- 1. Chang Baptist Church
All together there are 17 churches in Tuensang Town. These major Churches have adopted 3 other Churches and also network with the other Churches for PLHA Support and Care Programs.
Strengthening Coping Capacities
1. Clinic Based Care
Clinic-based care is being delivered to IDUs by three institutions - Chang Baptist Church, Khiamniungan Baptist Church and Eleutheros Christian Society.
2. Referral Care
Three doctors are attached to the Government Civil Hospital/ clinic.
Two counselors of ECS are also trained nurses.
3. Hospital Based Care and services - VCTC/ PPTCT
Two Counselors from ECS are attached to the VCTC of Tuensang Civil Hospital. One counselor is attached to the PPTCT of Tuensang Civil Hospital. Both pretest and posttest counseling is provided to all patients undertaking the HIV sero-prevalence tests.
4. Case Management Services
Overall Care and Support is provided under the care component of ECS. It includes financial support as well spiritual and emotional support. The NGO acts as a referral point for Community-based Care/ Hospital-based Care services.
5. Nutritional Services
ECS provides nutritional support for acute symptomatic cases at the homes or hospitals based on the criteria that the client has no immediate family/ relative’s support.
6. Home Intervention Programs
Counseling facility: Pretest and Posttest Counseling are available not only at the hospital where VCTC services are provided but counselors avail services to symptomatic clients unable to access hospital services. Intense follow-up programs for every client of ECS is undertaken.
7. Home-based Care Services
Doctor and nurses visits comprise an integral component of home-based care services. Opportunistic infection medicines are made available for PLHA. Free check-up facilities are made available and consultant doctors of the organization prescribe medication or cross-refer clients to RNTC/ TB programmes for those with cross infections. Free needles/ syringes/ condoms are provided to the clients, especially drug users. Cases with acute abscess and gangrene are closely followed up as part of home-based care services. Case managers follow up reported hospital cases at their homes once they leave the hospital. STD/ STI treatment cases are followed up at their homes. Bacterium prophylaxes are provided to PLHA and the case managers monitor patients on a routine basis for compliance and adherence.
8. Support Groups
ECS promotes social support group among IDUs and other High Risk groups including significant partners of IDU clients. The micro-credit/ thrift facilities empower them to become economically self sufficient and self-reliant. It has promoted entrepreneurship among the targeted population who have access to credit which is linked with the “Edou Bank” which allows groups to access 100 percent loan against their deposited amount. The groups nurture and promotes spiritual as well provides and enabling environment for social re-integration and acceptance.
Making Choices
The current intervention program offers an array of custom-built services designed to cater to the specialized needs of the IDUs. Given below is the list of various services that add value to the intervention efforts and aim at improving the quality of life of PLHA.
House Of Hope: Rehabilitation Center in Longphang.
The Organization presently conducts Behavioral Change Camps in batches with intense follow-ups of their clients through case managers (ORW).
Coffee House in ECS premises.
Drop-In-Center in Tuensang Town, offering rest facilities, reading room, counseling, pharmacy and referral services.
Livelihood Skills Unit providing skill training in Tailoring to positive high-risk group people as well as to those who fall Below the Poverty Line (BPL). This is done with the aim of providing self-employment options to positive people (who may have lost their jobs due to discrimination) and those who are economically disadvantaged to sustain their economic well-being.
Non- formal education NFE was imparted to all children of positive clients till last year. The program has since been discontinued envisaging admission of children to formal schools ensuring access to higher education, thereby leading normal lives.
Overcoming region-specific challenges
Intervention in other areas of Tuensang District by ECS:
Noklak Area
1. Targeted Interventions (TI)
Under TI programs a Drop-in-Center has been established, with 2 Peer Educators, 2 Outreach Workers and 2 Youth Counselors. Care services are undertaken through alliance network through 2 Counselors and 1 Outreach Worker placed at the KBCA.
Shamator Area
1. Targeted Interventions (TI)
Under TI program in Shamator there are 4 Peer Educators, 1 Counselor, 3 Youth Counselors and 1 Outreach Worker.
2. Government responses
Conducted primarily through the Medical Department, programs include Blood safety, VCTC and PPTCT, OI care, supply of drugs/ reagents, training of doctors. In the whole of Tuensang district VCTC and PPTCT facilities are available only at Tuensang Civil Hospital. Pretest and Posttest counseling facilities are provided in the hospital premises through ECS counselors. Blood Bank is not functioning at present. Medicines for OI are provided free of cost both at the hospital and at the ECS clinic. There is only one STD clinic in the whole of Tuensang District attached to the Tuensang Civil Hospital. Medicines are available for symptomatic cases and medicines for OI are provided free of cost to PLHA at the ECS clinic as well as the hospital. In the year 1998-99 the medical department conducted a State level training on Syndromic Management.
3. Behavior Change Interventions among HRG
In Tuensang BCC (Behavioral Change Camps) are conducted by ECS at their Rehabilitation Center (House Of Hope) in Longphang which is 25 Km away from Tuensang town. Support Groups among users/ex-users and their partners are initiated by ECS. The Targeted intervention programs as well the care component covers BCC Strategy.
4. Role of NGOs in VCTC and PPTCT.
General VCT approaches and issues according to ECS engaged in providing services:
Goals and Purpose:
- a.) Pre/ Post test (HIV/ AIDS).
ECS managed services are integrated to health care facility at the Government district Civil Hospital and VCT is allotted a counseling room. Care facility attached to the network of Community outreach of Alliance churches/ association also provides pre-test/ post test couselling through outreach network and home based intervention strategy.
ECS counselors are attached to the Civil Hospital Tuensang. VCTC/ PPTCT provide pre and posttest counseling. TI team (Targeted Intervention team) identify drug users and people in the high risk category (users/ sexually active/ wine brewers/ pregnant mothers who are in the HRG) and undertake door-to-door counseling, the high-risk groups are given counseling and encouraged to go for testing. In case they are willing to go for testing they are linked up to the VCTV/ PPTCT counselors. Each conformed positive case is linked to their respective churches (tribe-wise break up) and provided with care and support through the alliance network at Tuensang with five churches and 40 churches under the Khaimniungan Baptist Association.
5. Harm Reduction for Drug Use – De-addiction, needle exchange and BCC
The Government department as well as ECS in Tuensang district have initiated various awareness programs on HIV/ AIDS issues. De-addiction, BCC and needle exchange programs are taken up by ECS in Tuensang district.
6. Harm Reduction for Sexual Transmission - Safer sex, condom use
In Tuensang Town Support Groups are formed among people in the HRG. This group comprises of drug users (ex-users/ present) and their partners, people who had a history of being sexually active, such as wine brewers. People can also get access to condoms in the Civil Hospital and in the ECS.
Findings on rapid survey on condom availability in the three target areas show that condoms are not very much in demand even if they are provided free of cost. Even condoms provided to clients in the HRG are not always utilized. Condoms are purchased only by the youths (male). On an average a maximum of 41 packets are sold monthly in one community where the population is estimated to be at 28.304. Some areas reported even lesser sales of only as many as 25 pieces in a month (from one shop). 50 percent of the pharmacies expressed that condoms are not sold openly as the cover pictures creates embarrassment to both elders and children when both parents and their children go to the pharmacy to purchase medicines.
7. Care and Support of PLHA.
Currently, except for Tuensang Town where care and support is given to PLHA through ECS’s alliances with CACS no other area has any care facilities for PLHA.
Reaching Vulnerable Groups
1. Organizations and HIV/AIDS related activities
Various NGO’s in Nagaland are working with NSACS (Nagaland State Aids Control Society) in tackling the issue of drug/HIV/AIDS related issues. TI programs of ECS are funded by NSACS. A Drop-In-Center by Yingli Mission Center under the aegis of NSACS has recently been inaugurated in Longleng.
Tuensang District AIDS Control Committee under DACC (District Aids Control Committee) that is under the aegis of NSACS has been caring out IEC activities in all areas of the district. Some of the activities carried out by DACC of Tuensang include:
Inclusion of HIV/AIDS awareness education in the Sunday school course. Tracts in local dialects (6 tribes) have been distributed in all interiors of the district. Five representatives from each village in Tuensang were given training and money was also sanctioned to conduct awareness seminar in their own villages. Altogether a number of 212 villages were covered under this program. Concert/ Inter-school Oratorical competition/ Script writing/ Poster Making, Folksong/ Folk dance are some of the activities taken up by DACC of Tuensang. Trainings and seminars are conducted for different groups age groups in all areas of Tuensang district. A video program titled “HIV/AIDS in Tuensang, whose problem it?’ was produced and telecast.
2. Linkages and Networking
The Tuensang District AIDS Control Committee has tied up with 5 tribal churches to work towards HIV/AIDS related issue. ECS care components are linked with CACS, Tribal Hohos, Church Associations, Support Group networks with ‘Edou Bank’ (Farmers Bank) among IDUs/ HRG and VCTC/ PPTCT of Tuensang Civil Hospital.
3. Capacity building.
Efforts so far, trainings provided to various stakeholders within community.80% of the TI staff of ECS who are one of the most able and efficient workers are ex-users. Learning through exposure. Stakeholders from faith communities were taken to Thailand to learn and interact with ONCB on Drugs and Trafficking, to the Prime Minister’s Office in Thailand, UNAIDS office to interact with program officials, visited the Thaynarak Hosptital for Drug and Alcohol Abuse, Samcare program on Community care and intervention among the PLHA Thailand, the Organisation has trained counselors from CDTM Hongkong, ISAAC International conducts ongoing programs for training community care providers, such as to the Core Groups of Tribal Churches, and to ‘Teachers as counselors’ an on going Education program for schools and colleges. Advocacy for service providers for ‘Supply reduction’ in the community.
3.7 Assessing Responses
An overview of the various intervention efforts carried out this far by NGOs, the Government, Community Based Organizations, Associations, Mother’s Groups and Religious institutions among many others has made a dent in the HIV/ AIDS scenario with particular reference to IDUs. However, as has been observed, the efforts are inadequate in some measure and need to be scaled up to match the growing demands in terms of size of the problem in question. Especially, in the districts, where direct services provision may not be feasible, partner institutions may be involved extensively with the necessary logistical and technical support and monitoring mechanisms for efficient delivery of quality services.
There are certain areas where both the existing service providers and the community are at loss to provide expertise as they themselves do not have the option of further expanding the scope and range of services having been already stretched to a large measure. Such technical expertise may be drawn from external sources – even across the state/ district, training in due course a full-fledged expert team who can sustain the program. A Training Needs Assessment of personnel and target audience can throw light on the current skill requirements of the target audience and programs may be custom-made to fit such need.
Maintenance of organizational hierarchy with clear-cut reporting and decentralized structures need to be in place for smooth functioning of the program. Roles and responsibilities of program personnel also need to be put in place that would facilitate performance assessment and set the agenda for growth. This would also enable monitoring of program activities on preset performance indicators.
Planning and allocation of resources – financial/ physical and human – need to be streamlined among both public and private service delivery mechanisms. These need to be congruent to overall strategy and Project Implementation Plan (PIP).
Much more efforts are needed in the following areas:
Behavior Change Communication
Harm Reduction (condoms & needles)
GIPA (missing strategy in the area)
4. Needs
4.1 Broad Needs Of IDU
High Risk Groups Need for acceptance
One of the foremost needs emphasized by the PLHA and HRG Support Groups was the need for acceptance by the community, their family and their peers. They also wanted people to view HIV/AIDS as any other disease. The community as a whole has not been able to create an enabling environment for PLHA to disclose their status.
All Support Groups in the HRG as well as confirmed positive cases firmly stated…
“PLHA should be accepted by the society, people should come forward to render help to PLHA, they should not be avoided but accepted”.
HRG Support Group and PLHA of Tuensang Town
Only in Tuensang Town access to counseling facilities initiated by ECS and access to medical facilities like OI medicines/ VCTC/ PPTCT are available. Such is the stigma and discrimination faced by infected and suspected infected people that some want access to medicines only through ECS counselors.
Behavioral Data Needs
Throughout the state the typical problem of paucity of data and information – more so IDU specific behavioral data is
scarce or virtually absent. The only information that is available and reliable is the sero-prevalence rates being monitored on a monthly basis in all the districts and the state AIDS control society. However, such information is available after a long interval and interim data is unavailable – where such basic information is there no specific data exists pertaining to high risk groups or IDUs/ sex workers and women. Such information has to be culled out from other secondary or unpublished sources that may be only indicative of facts. There is a need for a good MIS to monitor target group specific behavioral data also pinning determinants of risk behavior and vulnerability to HIV.
STI / HIV Surveillance Data Needs
As highlighted above in the case of lack of authentic behavioral data, STI and HIV Surveillance data also is rather wide to interpret and such BSS cover the entire northeast with no state-specific or district specific indicators. What is thus needed is IDU specific studies monitoring the epidemic.
Training Needs/ Capacity Building Needs of target groups
It is felt that participatory training needs assessment would aid in developing skills of program beneficiaries and thus enhance response pertaining to IDU. The same may be replicated among other groups and focus on specific programmatic components that need to be handled on an individual basis.
4.2 Prevention Needs
Toward A Drug Free Life
Behavioral Change programs have to be integrated focusing not only among the users but also among the school children and out-of-school and college dropouts. Every community reportedly have a very high number of school/ college dropouts. There is a lot of fear, apprehension and misconception among school children who are aware of the social disorganization through drug abuse that is plaguing society. However, there is always the fear of them being caught in this fatal trap. Hence, they need to be educated early and thus be prevented from meeting the fate of their elders. During a Participatory Learning Appraisal (PLA) session with school children, in addition to the misconceptions spelt out by the children, the attitude of some students towards drug users was very aggressive and hostile. This may be attributed to lack of information.
Prevention-centered Needs
Going beyond awareness and BCC intervention needs both IDUs and stakeholders felt the immediate need for more drug De-addiction facilities combined with BCC. Increased efforts in Sexual health education among schools, for out-of-school youth, safe sex education needs, condom promotion needs, enabling environment needs (Creating Enabling Environment involves removal of disabling factors in environment – seeking to remove barriers to HIV prevention, as well as social, cultural, economic and other environmental barriers) enhancing advocacy needs, treatment of STI, need for Syndromic Management Training on STI at the periphery level were accorded immediate importance among the target population.
Need for IEC materials produced in local languages
An important aspect that needs to be focused on is harm reduction programs. Though all section of the community may not be in agreement about harm reduction measures like condom promotion and needle exchange program, we cannot deny that it is a need among the HRG category. Almost every section of the people the team came across have admitted to drug users as well as many sexually active people in their community. Despite being aware of the mode of transmission findings on Condom survey shows that it is not much in demand. Sharing of needles including of used needles thrown by the pharmacies and blood products are also common among the users.
More than awareness seminars and workshops there is need to integrate intensive targeted programs for targeted groups at all levels, which will reach people at the grass root level. Incomplete information is making the public more frightened and confused which is also giving way to stigma and discrimination. “We even fear helping our friends who hurt themselves when working in the fields”. Majority of the time Users always mingle with other fellow users and many of them are also very anti-social, hence, workshops and seminars on HIV/AIDS programs conducted in public places like Town Halls and Churches seldom reaches the desired group. “In-depth understanding of drug use and how it is interrelated with HIV/AIDS which will remove social stigma and in turn enable an environment for acceptance of PLHA”- one of the needs identified by Kiphire Community.
The cost of Syringes was one major indicator to risk behavior among the IDUs. “The cost of syringes is Rs.5 and so sometimes it is hard to spend that amount after spending the whole amount of money to arrange for the stuffs”. An incident, related humorously, pointed to high drug use and how they continuously supplied their stock, (when they were using drugs and studying), “We dispatched parcels by ‘registered post’ containing drugs to our own names and on the cover we used to scribble “Happy Birthday” to cheat the authorities”. (into making them believe that the parcel contains a gift and not drugs).
4.3 Care and Support Needs

Basic Needs
These pertain to basic needs of IDUs as perceived essential for them. The intensity of the need depends on the economic situation, external support received, familial or community support and extent of infection (that may have an impact on the physical and psychological bearing) of the person concerned. Specifically, such needs relate to Nutritional, Shelter and need for Special homes for long-term rehabilitation (in the case of IDU they mean de-addiction centers.
Medical Needs
IDUs have expressed the need for free tests and diagnosis and treatment. Currently VCTC and PPTCT centers are being accessed at district level, the same are not available in remote places and hence IDU face problem of increased costs, poor accessibility due to distance and bad terrain typical of Nagaland and inclement weather. They also are concered about home care facilities for children and dependents (spouse/ parents/ children) . More importantly is the concern about availability of affordable, consistent supply of ART Treatment, free diagnosis and treatment (of STIs and OIs) and syndromic management.
All PLHA expressed the fact that one of the motivating factors that encouraged them to go for testing was the belief that they can get access to medicines which can prolong their life.
Knowledge Needs
Awareness at the School level is the primary task in such program interventions. Focusing on the younger generation, through formation of core groups among school children with the involvement of school authorities, teachers and parents, it was believed is the need of the hour and would have more far-reaching consequences in quelling the tide of IDU behavior in the state.
Apart from basic literacy enabling them undertake self-employment ventures and be economically independent, treatment literacy is very important as many are illiterate or drop outs and undergoing de-addiction or rehabilitation requires taking the right medicines in the right dose supplemented with diet and other safe behaviors. This apart, IDUs also felt that an area of gap was the absence of life skills and need for augmenting such skills to lead a better quality of life.
Economic Needs
A member of the PBCA opines, “If only the user (IDU) suffers it is another issue, but the entire family suffers, and even after they die they leave a legacy of suffering”. (that is obviously difficult to come by). Few families who have managed to send their children outside for rehabilitation but did not meet with expected success, as follow up programs were practically non-existent. Almost every second family is facing an addiction problem - some have even two addicts. Out of sheer frustration, few parents have reportedly lament to their sons with drug dependency, “Please take the drugs and die, and at least when you die we’ll have some peace, as we feel that whatever we have done has been in vain”. In some cases both husband and wife are addicts. There was a case in a particular community where the father passed away and there was no place to bury him as the son had sold off their ancestral property. Thefts as well as extortions are a common feature leading to disputes creating an atmosphere of ill will. Shop owners and pharmacists have enough reason to complain. According to the Chambers of Commerce, Longleng, “We have to close our shops early (4 p.m.), the demands of the addicts even come down to as low as Two rupees for a vial/ drug and non locals traders are threatened more”. Addicts also end up with the habit of selling every thing they could get hold of – ranging from clothes, household goods and even livestock. Lack of unemployment also contributes to the drug scenario. It is estimated that 5 percent of drug peddlers in Longleng depend on this trade as a means of livelihood.
IDUs expressed a sense of discontent with the poor response of government and others with regard to provision of technical know-how for Livelihood Management Programs. they also preferred managerial and financial assistance for undertaking self-employment ventures. IDU were surprised at the non-formation of Self Help Group among IDUS, in their respective places and have an unfulfilled need of accommodating HRG, PLHA and involving them in sustainable income generating activities.
Psychosocial Support Needs
Individual and Community Acceptance
The process of healing can only start when PLHA and the community come to terms and the community accepts his/ her status. The family along with the community should take the responsibility and work towards enabling an environment for the PLHA to get access to financial, emotional, and spiritual as well as medical support including access to drugs and medicines, counseling and other services.
Next to being accepted within the family, IDUs expressed the need for recognition of their status in the community and larger social set up. The lack of professional support and services such as counseling and guidance including referral services in a long felt unmet need according o respondents. Finally, PLHA wanted to participate on issues concerning themselves (GIPA principle), forming, managing and sustaining Social Support Groups to enhance their social security and augment conflict resolution.
Social Acceptance Needs
By social acceptance unfulfilled needs what IDU meant was removing stigma and discrimination, partiipation of PLHA in social activities and societal, community and family support to PLHA in all that they do.
Legal and Human Rights Needs
A visit to the Tuensang jail where the research team met 7 IDUs brings out the pathetic plight of the inmates many of whom suffer from withdrawal symptoms. There is no recreational facilities, no proper beds (they are made to sleep on the floor in biting cold), with no access to medicines and prisoners – invariably IDUs - are locked up the whole day in confined dingy cells. This also calls for examining law-enforcing bodies with respect to human rights violations.
Spiritual Needs
What has been observed in Nagaland is that the Church is a powerful institution and capable of bringing within its fold IDU and other HRG, being able to provide rehabilitation also. The role of Faith Based Organizations (FBOs) has been prominent with PLHA resting their hopes on unclenching Faith in God, Caring (toward fellow brethren) and Love.
4.4 Institutional Needs
Respondents hailing from the Longleng Community felt the need for trained counselors to work at the grassroots level among the users to minimize drug use/ stop further spread/ know their grievances/ problems/ frustrations and identify their needs.
The Kiphire teaching community (both Government and Private) identified the need for trained counselors in schools. Time factor in finishing the lengthy school syllabus makes it difficult for the teachers to concentrate on the emotional aspects of a student. According to the teachers 60 perent of the student population of Kiphire Town is from the villages. They either stay with their relatives or stay in rented places thus being reprieved of emotional and psychological support, which could promote risk behavior among the youth population, devoid of parental care and guidance or familial control.
Economic empowerment through Institutional Needs
PLHA felt a sense of urgency in fulfilling their immediate economic needs through income generating activities: Many were of the view that sustained economic activity can go a long way in managing basic, yet expensive economic needs such as medicines and nutritional needs.
Every community in Tuensang district is in dire need of targeted intervention programs and a rehabilitation center in one’s own locality that can foster easy access. The economic condition of the family too deters them from seeking treatment outside. Years of accommodating an addict in the family invariably drain the entire resources of the family as well as the economic base of the community. Families have reportedly lost their entire life savings. Many parents are fed up and have almost given up hope.
The women in the HRG category wanted to have more Support Groups among the vulnerable category of the population so that within the group they can support the children of infected parents when the parents are no more or render physical and financial support when the parents are unable to do so. Economic resource is not the prime factor to reach out to others in life, and members belonging to Support Groups bring this truth home to others. Almost all of them fall in the BPL category. Many realized and shared about the importance of being a part of a Support Group.
“We want to avoid drugs, thus in order to support one another we formed this support group. Being a part of this group also helps us to carry on without having a relapse”. “We are seeing to the schooling of one of our friend’s child, and when ever there is a surplus we give it to the most needy member in our group”
– Women Support Group (HRG), Tuensang.
While interacting with one of the Support Group of Tuensang the group brought out the need for recreational facilities in the locality. Though they have land they do not have adequate resources for the necessary infrastructure.
The Longleng community emphasized the need for a hospital and a rehabilitation center for the users. There are no intervention programs visible though programs are said to exist. The is dire need for intensive intervention as there are reportedly (mentioned by NGOs and MOs) many drug users as well as many drug /HIV/AIDS-related deaths are on the rise in Longleng. The Noklak community emphasized on the need for proper communication and transport facilities, more outreach workers with CACS as well as access to medicinal facilities. In Shamator the Community’s emphasis was on the need for trained teachers in schools, access to medical facilities and a hospice for PLHA. In Kiphire apart from intervention programs and the need for rehabilitation center there is a need to identify gaps and build up grassroots level contacts with the end users. It has been observed that no group or individual have been able to penetrate the circle of the users.
Need of Rehabilitation facilities In Government Institutions
Lack of extensive rehabilitation measures by the Government or in partnership with private sector is considered a major barrier in preventing HIV/AIDS. In Nagaland the law implementing agency as well as the underground faction catches many users but this practice is often discouraged in the Police Department, as there are no facilities to rehabilitate them. In fact the Government is not able to provide even basic needs to the prisoners.
Institutional Capacity Building and Training Needs
Discuss need for capacity building and training different types of organizations in got, private and community, involving existing community organizations and traditional governance structures, developing linkages in each of the 8 areas, improving medical infrastructure and supplies.
From the point of IDU who are now PLHA, realization and recognition of the intensity of the problem has been too late. Almost an entire generation as well as the next has been lost. No individual or organization or government alone at present can shoulder the responsibility of care and support of PLHA. The entire community has to be activated to the grassroots level to come forward and be a part of the healing process.
The IDUs have identified critical individuals and areas that require fresh and sustained impetus – such as need for training medical doctors on not only clinical research and advances in HIV/ AIDS but also in attitudinal disposition with the patients, training of other health care practitioners including traditional healers, professional social workers and paramedical staff in providing care and support services for AIDS infected persons. The PLHA also expressed a change in attitude of the Government machinery and personnel to HIV/ AIDS and those affected by it. Other areas of specific training that they recommended included Focus on Environmental Needs (disposal of bio-hazardous wastes) and Harm reduction programs/ BCC/ needle exchange programs. They also recommended that more awareness on various clinical and social manifestations of HIV/ AIDS may be done at the grass root level through NGO’s efforts. IDU from Longleng opined that there needs to be immediately a research or proper survey about the drug/ HIV/ AIDS scenario in Longleng district. They also suggested that NGO’s, State Government, Health workers and Religious Bodies should also come forward to address this problem. They expressed concern and the need to identify gaps and build up a rapport with the users through a trust building process.
4.5 Health Infrastructure
Longleng District
1 specialist/a gynecologist/ a surgeon/4-5 Medical Officers /sufficient medical attendants..
Lab technician/more than 10 nurses
Kiphre District
Surgeon /a pediatrician /an Anaesthetist /a gynecologist/ 5-6 nurses
Infrastructure Needs in Longleng
Blood Bank (under process).
Detox Center for IVD’s.
Requirements for STI Clinics: Full reagents, Dark Ground Microscope.
CD4 testing facilities.
Proper communicable roads/telephone facilities.
Provide staff quarters/Medical colony.
Proper infrastructure in the PHC – Enough and proper space to cater to the patients/operation equipments/sterilization facilities/lab equipments.
Blood Bank/VCTC/STI/PPTCT facility.
Proper water supply (maintain the pipeline)/regular power supply or at least a generator/fuel to run the generator/refrigerator to store blood.
Infrastructure Needs in Kiphire
Blood Bank/VCTC (a must)/PPTCT
An X-ray machine/a technician/bare minimum facility for routine examination/direct water connection.
CHC of Kiphire District is a 50-bedded hospital. But according to secondary sources most of the hospital furniture’s are broken. Due to shortage of manpower they do not maintain a separate STI data.
There is no PPTC/VCTC/Blood Bank facility or DACC. There are many users in dire need of access to medical care in Kiphire.
The medical facilities of Longleng including trained manpower and infrastructure are in a deplorable state. There is shortage of Health Care Providers. For the last 15 years only one MO has been in station. Other doctors reside only on temporary basis. There are no medical quarters for the hospital staffs. In the 30-bedded Community Health Center upgraded three years back there are only five health care providers – one MO, two staff nurses and two ANM (auxiliary nurse midwife). There is also a 20-bedded THW (Temporary Hospital Ward-Leprosy) but no doctors have ever been in attendance. Lab facilities are there for routine blood examination but the technician is never in station, the MO has to see to it. There is not enough space/proper space for the doctor/patient/erratic power and water supply/no generator/no refrigerator to even store blood/no-testing facilities to confront suspected cases. Due to acute shortage of manpower no data has been maintained, OPD procedure is followed as there is no time to even register the patients.
5. Resources Available
The presence of NGOs or grassroots organizations in Nagaland is significant though it may be observed that the number and concentration of NGO efforts are more concentrated in urban areas – District Headquarters and small towns. They need to expand their activities into rural and remote districts/ areas as well as the epidemic is now taking a generic course and affecting the entire population. Moreover, in rural areas, NGO services, especially care and support for IDU are required providing professional, complete range of facilities especially to improve the quality of life of IDU PLHA .
A glimpse of the organizations also reveals that they are a blend of religious, cultural, socially conscientious persons, responsible women seeking social change and even activist groups. With such a diverse background and local foundations, the organizations have formed a good rapport with the target population – the IDUs and working for specific activities in each region. The range of activities include provision of community-based rehabilitation, diagnosis and medical treatment facilities including drugs and medicines and tests, professional services such as counseling and referrals and follow-up, economic rehabilitation through linking with resource providers such as banks/ cooperatives for financial support, social and community support mechanisms through a combination of faith, sports and cultural activities. Redress of grievances in the community and initiating dialogue and discussion with stakeholders concerned also satisfies the GIPA principles giving PLHA the twin-advantage of empowering PLHA as well as removing stigma and discrimination, thereby integrating them into the mainstream.
Organizations such as Eleutheros Christian Society. (Tuensang), Phomla Hoichem. (Longleng), Association of Phom Graduates and Officers (Longleng), Yingli Mission Society (Longleng), Helper Samaritan (Longleng), Women’s’ Welfare Association/ Working Ladies. (Kiphire Town), International Border People Welfare Organization under the aegis of NSACS. (Kiphire town) and Tuensang Public Forum. (Tuensang) are undertaking various activities depending on their resource availability and operational capacities. However, there exist a few gaps in their operation that calls for a need focusing on increased resource generation, building of organizational strengths (technical, managerial and financial skills) and structures, decentralizing efforts, enhancing capacities through training and input of skills.
The Church, especially the Baptist Church that is prominent in Tuensang and other intervention areas has a very important role to play in settling community issues (as Christianity is the binding force) and improving the lot of IDUs, mainly those in need of immediate care and support as well as potential IDUs so that prevention today can stem the tide of the epidemic as has been proved in many countries faced with a similar situation. The following pages provide the list of all the possible resources.
5.1. Community Organizations and Structures
|
Eleutheros Christian Society. (Tuensang)
|
Eleutheros Christian Organisation a non governmental organization registered on March 1993. A community based organization working in 16 villages covering two development block. Works in the area of Rural development, educational reforms providing 22 support teachers in government schools covering three blocks mainly, the Sangsanyu block, Noksen block and Noklak block. The organization works with Action AID and IGSSS on rural health, education, community development on IGP, Food for work programmes, livestock rearing, Self Help Groups- Micro/thrift saving groups among women and men farmers. Other areas of intervention includes Targeted intervention with NSACS/NACO include covering 8 towns and 129 hotspots covering all major tribes namely the Yimchunger tribe, Khiamniungan tribe, Changs, Sangtam, Ao, Sumi and other non local communities in the project area. The organization has components on Community care an alliance network with five churches and two tribal associations. The programme covers more then 1000 IDU’s and High risk Groups. Provides VCTC and PPTC in collaboration with the district hospital at Tuensang. Established a network of Self Help Group in 40 villages with more then 400 groups and 200 affliated to the organization for banking purposes. |
|
Phomla Hoichem. (Longleng)
|
Phomla Hoichen the apex women body of the Phom was established on 9th May 1992. It started with 42 members. It comprises all Phom women who have attend 15 years of age. The organization’s motto is “Ray Of Hope” and its main objective/activities is empowering the women folk/to fight social evils/go from village to village to provide relief during natural calamities/disasters/hospital visits. The organization has a holistic ministry approach and has been responding to the community’s need of the hour. In January 2004 they had established network with ECS on Targeted intervention among IDU and HIV/AIDS programme. |
|
Association of Phom Graduates and Officers (Longleng). |
Established in 1991. All the graduates and officers of the Phom community is its member. An elite body of intellectual section of the Phom community that charts the future course of the Phom tribe. Comprises of 34 officers and 25 post-graduates and 500 graduates. The aim is to bring socio-cultural and economic development within the community. The APGO established the Yingli College in 1992 as its first venture. Organizes programmes on HRD, education awareness seminars, literacy campaigns etc. |
|
Yingli Mission Society (Longleng) |
A non-governmental organization in Longleng Town. They run a Drop-in –center under NSACS and has one peer educator under Kripa Foundation. (Governor’s incentive). |
|
Helper Samaritan (Longleng) |
A non governmental organization which initially begun as a Volley ball club. Changed their name and objective in 2002. Started survey with the District AIDS committee in 2004 January to disseminate awareness on HIV/AIDS. |
|
Women’s’ Welfare Association/ Working Ladies. (Kiphire Town).
|
Advocates for access to women schemes, networks with government, social support system. Willing to collaborate with ECS on HIV/AIDS in their community. |
|
International Border People Welfare Organization under the aegis of NSACS. (Kiphire town). |
By the support of Nagaland State AIDS Control Society involved in interventions among IDUs in Kiphire town. |
|
Tuensang Public Forum. (Tuensang). |
The organization was declared on 1st October 2003. It comprises of all the tribes of Tuensang District and representative from all the sectors. The aim and objective was to strengthen the overall activities of various stakeholders. It a pressure group for the public and ready to address HIV/AIDS issues and combat in reducing supply and demand of drugs. |
|
Shamator Women’s Organisation (Shamator) |
All women in Shamator town are registered members of the organization. Objective was to organize khels (sectors) to control illegal actives of youth. Empower and educate young women and youth population to refrain from indulging in anti-social behaviours. |
5.2 Government departments and local governance structures
|
DACC (District Aids Control Committee) of Tuensang. |
Involved in HIV/AIDS IEC programs. The Committee comprises of the Deputy Commissioner as the Chairman. Cover the whole district on dissiminating information on HIV/AIDS. |
|
Red Cross Society- Tuensang Branch |
Started Polio immunization in the 80’s. Provides relief during natural disasters/calamities and provides assistance to the hospital and Jail inmates on occasions like Republic Day and Independence Day. Enabled to help open a Red Cross Center at Longleng. |
|
PHC (Primary Health Center) Shamator |
A Primary Health Center with 1 Doctor and a total strength of 41 HCP. Under Smator PHC there 4 Sub-Centers. |
|
Health Facility CHC - (Noklak) |
An 18 bedded Community Health Center. With 2 doctors, 10 number of nurses with total hospital staff strength of 46 members. No sterilization facility, no kits such as auto-clave, Operation not completed. A non-functioning X-ray machine. |
|
Tuensang Civil Hospital, Tuensang |
VCTC/OI/PPTCT/STI clinic facilities (pre and post counseling). Blood Bank (under process)/Regional Diagnostic Center under construction |
|
CHC- Community Health Centers (Longleng). |
A 30 bedded community Health Center, upgraded 3 years back. 2 staff nurses and 2 ANM. Under the CHC there are two sub-center in Sakshi area, 1 Sub-center in Longleng, 2 sub-center and 1 PHC in Yongya area. 1 dispensary and 1 PHC in Tamlu area. Temporary hospital ward (Leprosy). 20 bedded hospital with no doctor. |
|
DRDA – District Rural Development Agency, Tuensang district |
All the center support schemes such as primary health, rural shelter, drinking water supply have been given to the villagers on subsidy rates through the VDB (Village Development Board) which is recognized by the board. The Dept also collaborates with State Bank for SHG schemes. The State Bank provides the funds. Two types of schemes: 1) SHG (Self Help Group) under this scheme there are 25 schemes (fisheries, knitting, weaving etc). 2) IHG (Individual Help group) this scheme is meant for the poor who are graded into different categories. |
|
District Sports Council |
The Council is responsible for organizing any sports events/tournaments in collaboration with the Dist Sports Officer. Earlier sports equipments were distributed freely to clubs/orgs but is presently defunct due to shortage of funds. |
|
District Welfare Officer |
Schemes under the Dept – Old Age Pension (Rs 100 per month) for 65 years and above, provides them with Identity Card so that they can get access to some concessions. Aid to disabled people – (Rs 75 per month) unemployed disabled people can get access to Individual loan (Rs 50,000 no subsidy). Travel concessions up to 50% are also given if a person is 50% handicapped/Scholarships for poor students (Rs.75 per month)/ICDS for both mother and child(nutritional packages) for people living in BPL/SHG schemes (grant-in-aid) 1 orphanage in Tsuwao in Noklak Dist looked after by Red Cross Society and 1 SHG in Sangsangyu/Tribal Welfare Program (construction of a residential school in Tuensang under the Central Board of School Education)/financial assistance of Rs 100 to destitute women/2 women hostel |
|
Yimchunger Women Organisation. |
YWO was established in 1959 and has a total staff strength of 14 personals. The activities are carried under the women secretary, women evangelist, mission secretary. The women department mentors the education section. |
|
Chang Women Society. |
Working Women’s Hostel is funded by the Ministry of social welfare. This is under construction and is due for completion wihin June 2004. It is hoped that the facility will cater to the need of single women who have no access to proper facility of stay and lodge. |
|
Tuensang Mon Public Organization. |
This Organisation is the apex body that comprises of five major tribes namely the Khimanyungans, the Sangtams, the Yimchungers, the Konyaks and the Changs. This is also to inform that these were tribes which were initially part of the erstwhile NEFA.(North Eastern Frointier Agency). The formation of Nagaland was essentially the merger of the Tuensang Division of NEFA with that of the Naga Hills Assam. The Organisation is headed by the President and the Executive Chairman. |
|
Tuensang Town Committee. |
The Town Committee was established in 1980 and has18 members out of which 12 is elected members and 6 are nominated members. But currently there has been a rise of 2 more elected members. The committee covers sanitation programmes for the whole town. They supervise trade license and prepare pricing for essential and commercial goods. |
|
State Bank Of India – Tuensang Branch. |
The State bank of Tuensang comes under the Regional office in Dimapur. The Bank consist of 1 Branch Manager, 2 Deputy Managers, 4 asst. managers, 9 asst. clerks, 3 ordinate staffs, 1 part-time sweeper. There are 6000 account holders in this Bank. They provide two types of loans, mainly- Bank regular scheme, Govt. sponsored schemes. Provides loans such as agricultural loans for farmers and SHGs schemes ranging from Rs. 50,000 onwards. |
|
Co-operative Bank – Tuensang Branch. |
The Head office is located in Dimapur and the sub branch is located at Kiphire. The Bank comprises of 1 Branch Manger and 10 staffs. The bank has 30% investors out of national average (1000 customers). |
|
State Bank Of India – Longleng. |
The bank comprises of 1 Branch manager, 4 staffs including 1 cashier and 2 sub-ordinate staff. The Banks provides various facility such as general banking, government sponsored loans. Sponsers 10-12 SHG’s. Provides loans ranking from Rs 50,000 to 1 lakhs at 11% interest. |
|
State Bank of India – Kiphire. |
The Town of Kihpire was initially a sub division of Tuensang. It is now a full fledged district as of 26th Jan 2004. The bank was a branch unit of the Tuensang branch. It serves only as a facility to transact Governmental funds and to cater to Government aided loans under the rural development programme. |
|
Police Dept of Longleng (under SP of Tuensang). |
The department is directly under the S.P of Tuensang. It consists of 1 SDPO, and has total 49 staffs- armed and civil. |
|
Police Dept of Tuensang. |
There are 5 police station under Tuensang district. Longleng, Longkhim, Noklak, Shamator, Tuensang and four sub-Police station in Tamlu, Chare, Noksen and Thonknyu towns. |
|
Excise Department: Tuensang
|
Excise Department is under the Superintendent Commissioner. The total strength of the department is 25 personals. It carries out the NDPS Act 1985 and NLTP act 1989. |
|
Goan Buras (GB’s)
|
Shamator: Though considered a town it still continues to be a suburban township where elders play a key role in the governance of the administration. Here the Gaon Buras are key agents of the state machinery. Tuensang: Is an organization which comprises of GB’s from all the sectors in the town. |
|
Doabshis (DB’s) a). Shamator b). Noklak
|
Shamator: Dobashi essentially means an Interpreter. During the British raj there was the need for people to interpret for which the post was created. Later this also meant administrative representation of the British. With time this post was amalgamated into the Government establishment to help the local administration and to serve as a customary court of law. There are 5 dobashis attached to the Administrative officer in Shamator. Noklak: Under Noklak there are 9 Dobashis. Tuensang: Comprises of six major tribes of Tuensang, namely the Sangtam tribe, the Chang tribe, Yimchunger tribe, Khiamniungan tribe Phom and Sumi tribe. They cover Tuensang Headquater and four other major subdivisions, Shamator, Noklak, Longkhim and Noksen. There are 37 DB’s under the Deputy Commissioner, Political Asst. To Dy. Commissioner. The DB’s are appointed under various category such as Special grade DB’s, Grade 1 and 2 appointees, contingency appointees who are under fixed pay. |
|
Khiamniungan Tribal council. (KTC Noklak)
|
The Khiamniungan Tribal Council consists of 10 Executive members. It covers 35 villages under India and 155 villages under Myanmar. They have adopted resolution to Control Drugs related issues within the community. The organization imposes fines on peddlers at Rs.20000/- and sends them for reprimand custody or incarceration by the Police. Addicts are imposed fines of Rs. 500 and send to jail. Joint Action Committee an inter-sectorial collaborative efforts to deal with Drugs and HIV/AIDS issues by the community. |
|
CKS- Chang Khulei Setchang (Chang Tribal Council). Tuensang Town.
|
CKS covers entire Chang area, approximately 50 villages. Under its jurisdiction the non residents. Changs in various parts of the State are also covered. The Office bearers is selected if she or he is from the Chang community. |
|
HOB – (comprising of three villages-Hukpang, Orangkong, Bhumnyu-Longleng). |
The HOB comprises of three villages, visibly Hukpang, Orangkong, Bhumnyu villages which contributed land for the establishment of Longleng town. It has been in existence for the last 20 years. The main activities to maintain law and order in the town. They cooperated with the government and check the flow of alcohol and drugs. Networks to get information, sanitation,, action against offenders. |
5.3. Churches and religious organizations
|
CACS (Churches Alliance For Community Support) -Tuensang. |
A care alliance under ECS with 5 churches and two associations. Each church has core group members selected from within the local community. They act as a support unit for PLHA and mentors the activities which are church based. |
|
Pastor’s Union - Tuensang Town. |
The Pastors Union of Tuensang comprises of the 17 Baptist churches of Tuensang. This excludes the Roman catholic and other denomination. The Union is a very strong lobby which has much say in the Town. The Government has on many occasion sought the assistance of the Union, particularly on issues pertaining to conflict and tribal clashes. The Pastor of the Yimchunger Church is the President. |
|
Pastors Union – Kiphire Town. |
This is also the union comprising of the pastors of all Baptist Churches. This is a strong lobby in the town. |
|
CACS – Noklak. |
This is the Care unit of ECS based in Noklak. This project is done in collaboration with KBCA which is the apex body of the Churches of the Khiamnyungan Tribe. |
|
Pastors Union – Noklak. |
As in the case of all the unions, the Pastors Union in Noklak is a union of the Baptist Churches of Nokalk. |
|
YBCA (Yimchunger Baptist Churches Association- Shamator)
Drop in center through ECS. (Shamator) |
YBCA started in the year 1950. The present strength of the staff is14 under different departments. The association has a Youth dept, Women dept, and the education section, which is looked after by the women secretary. Resources under YBCA: Institutional Resources: Shamator English School/Nimi English School/Shalomi English School/Pinkhim English School/Sunday School/Kihoto Theological College.
On going programs with CASA (Churches Auxiliary for Social Action). A house under the Women dept is rented out. Livelihood Management through income generating activities like -, teak and bamboo plantation as well as horticultural products in more than 50 acres of land. |
|
PBCA (Phom Baptist Christian Association) Longleng. |
PBCA the apex Church body of the Phoms is in the 51st year of its existence comprises of 42 churches. The Association has a holistic approach in its ministry and is involved in diversified fields. Their area of work involves Youth Ministry, Sunday school ministry, Child Care, Support to Missionaries, Literature Society, Community Developmental work, Education, Livelihood Management programs and intervention in Noklak and Burma. Earlier the Association has also worked with World Vision, EZE (Germany) and The Leprosy Mission Of India. Presently the Association has on going programs with the Holistic Child Development Of India. Resources under PBCA: Phom Lampong English School/Guest House/Weaving Unit cum training center/ Carpentry Unit/Orphanage (120 children are currently residing in the orphanage). Lempong Clinic/Self Help Groups/Grain Bank/Constructed 18 school buildings (1 high school, 4 ME school, rest is primary school). Constructed water tanks and reservoir in all villages of Longleng District Currently focusing on plantations and Fisheries (developing stage) to support Mission Field. |
5.4. Private sector/ Student Body/Unions
|
Edou Bank- Under ECS Tuensang. |
The Edou Bank was initiated under the aegis of ECS, to facilitate banking within the Self Help Groups. The Edou bank is localized banking run by the SHG’s in Tuensang town, Tuensang Village and Hakchang village. It was formed in Tuensang town on February 2003. The SHG Federation members are represented as the executive member of the Finance committee. There are eight finance committee members selected by the respective local SHG’s. The Edou Bank avails loans at 100% against the total investment of each group. The interest of the loan is returned as a dividend to the groups that deposit the amount to the bank. There are currently 43 SHG investors and provides loans ranging from Rs.10000/- to Rs 85,000/- at the rate of 2%. |
|
TMSF (Tuensang Mon Student Federation). |
As is the case with the TMPO, the TMSF was initiated with the view to bring together the student community of the two districts Tuensang and Mon to a common platform. The body was instrumental in lobbying with the Government on many issues. In the initial years it even moved for the creation on Tuensang as a Union territory since the forward tribes continued to marginalize people of the two districts.. |
|
Chambers Of Commerce – a).Tuensang. b.) Shamator. |
a).Tuensang: There are 42 active members in the Chamber of Commerce. The members constitute of locals as well as non-local. The non-local are residents from U.P, Bihar, Rajasthan, West Bengal and Assam. b). Shamator: The office of COC was inaugurated on 10th January 2004. It was set up to support and help business community during accident cases, extortion issues. They are represented by business communities from Assam, Rajasthan, Bihar, U.P and local merchants. c. Longleng: It was established in 1982.The union was formed as a support system, to address communal disharmony, conflicts among local and non-local residents. |
|
USSC (United Sangtam Student Committee) Kiphire. |
The Sangtam tribe most interestingly is spread over two districts. Most of them are in Tuensang and a major presence in Kiphire district. The USSC is the unit oragnisation covering Kiphere town. |
|
All Student Leaders’ of Kiphire District. |
The All Student Leaders of Kiphere is the collective body of student leaders of kiphere district. This brings together people not only of the tribes present in the districts but of all tribes having its presence in the district. |
|
Working Ladies – Kiphire. |
It is a union of all Government working women and also the non-governmental agencies. It is a platform to address to grievances of women in particular and to serve as a forum to address to the welfare of women in the district. |
|
Private and Government School Teachers- Kiphire. |
Most unions of schools segregate Government run schools from private institution. In this case in Kiphire the union not only caters to one section but to both which in a sense brings cordiality and also quality in delivery of services. |
|
Chambers Of Commerce – Kiphire. |
The Chamber of commerce |
|
All the Student and Village Union and Churches of Longleng Community. |
|
|
Khiamniungan Student Union - Noklak. |
|
|
Mother’s Association – Noklak. |
|
|
Chambers of Commerce – Shamator. |
|
|
Yimchunger Women’s Organization – Shamator. |
|
|
Mobile Union of Noklak |
|
5.5. Others:
Community Resource location
|
Land to be donated by APGO of Longleng district in case of intervention programs related to drug/HIV/AIDS programs. |
Longleng |
|
Land to be donated by the GB’s Union of Kiphire District for any intervention programs related to HIV/AIDS program. |
Kiphire |
|
Local Ground/church buildings/school buildings/Town halls (in all research area). |
|
|
Every family have own field in Noklak/land is abundant. |
|
|
Christian High School |
Noklak |
|
Agape DIC (Drop In Center) |
Noklak |
|
K. Theological College |
Noklak |
|
Bible School |
Noklak |
|
Mission School |
Noklak |
|
Mind Adventure Group – NGO |
Longleng |
|
Yingli College (private) |
Longleng |
|
Puissant Club- Support Group Shamator. |
Puissant Club comprising of 34 users formed in the year 1999. Majority of the Club members are employed and manage on individual contribution. The members are all IDU’s or alcoholics who want to show to the society that they too can contribute something. The Club is sponsoring a pastor in Pungro area and also assists theologians. The funds are utilized to help the poor during times of sickness and death. |
- 6. Building Consensus for Action
The consensus process began with the different consultations during the study. A local stakeholders meeting was organized and the proceedings of the meeting are presented in this section. Further stakeholder meetings with participation of donors, FHI, NACO, NSACS are needed to evolve a Expanded Comprehensive Strategy .
Report on Multi Stakeholders meeting on Comprehensive situation Assessment on HIV/AIDS and responses in Tuensang, Longleng and Kiphire districts held at ECS Office on April 20th 2004.
It was a rare occasion when political, religious, Government and Community representatives and leaders from different got together to discussed HIV/AIDS in Tuensang and decided to work together for prevention of HIV/AIDS and Care and support of HIV infected.
 Family Health International (FHI), India Country Office, New Delhi an international Voluntary Organization is working with National AIDS Control Organization(NACO), New Delhi, and Nagaland State AIDS Control Society (NSACS), Kohima through Eleutheros Christian Society (ECS) Tuensang to carry out the Comprehensive situation assessment on HIV/AIDS in Tuensang District including the newly formed Districts of Longleng and Kipheri.
Family Health International (FHI), India Country Office, New Delhi an international Voluntary Organization is working with National AIDS Control Organization(NACO), New Delhi, and Nagaland State AIDS Control Society (NSACS), Kohima through Eleutheros Christian Society (ECS) Tuensang to carry out the Comprehensive situation assessment on HIV/AIDS in Tuensang District including the newly formed Districts of Longleng and Kipheri.

The assessment is studying the situation current responses, needs and available resources to help plan future efforts in controlling HIV/AIDS in the District the field work of the assessment has been completed by the ECS team and key findings and implication were discussed and presented at the Multi Stake Holder meeting held at ECS Office, Tuensang on April 20th 2004.
The meeting was chaired by Mr. Chingmak Kejong and inaugurated by Hon’ Minister for Education Mr. P.Chuba Chang. As a symbolic act of Cooperation, Mr. Nungsanglemba the president of ECS welcome the minister and said that though there may be personal differences, he appealed that we have to come together to side with those who have become the victim of HIV/AIDS and to work towards prevention. The minister mentioned that though Tuensang district was among the highest prevalence district, the facilities for treatment testing and care was limited. He assured that he will do his best to ensure that the government provides urgently need Anti-Retroviral therapy for HIV infected persons and the necessary testing and other facilities including CD4 count machines. He said, “I will fight for this issue but I would need communities support”. He urged different Stakeholders from different tribe, departments and organizations to work together to combat HIV/AIDS in the district. He appreciated the efforts of ECS in creating awareness among many sections of the society and providing care and support to infected persons and people with risk of infection. He urged the FHI Consultant to take back the message to Delhi about needs of the District and report the situation that he has observed. Some quotes from the Minister’s inaugural address:
“We don’t want our Children to die-the present generation to die of HIV/AIDS”
“We are a permissive society so we need to used preventive measures”
“Why go to Kohima? We have to fight for access to medicines, ART and CD4 testing facilities in Tuensang.
“I will fight but I need your support”

Following the Minister speech, Mrs. Phutoli S. Chingmak presented to the house the findings of the research team and thanked all the people of all the districts for welcoming and cooperating with ECS during month long research. She also informed the house that in few places the community even offered land and resources to initiate work and this we feel is an indication of community preparedness to respond to the problem.

Five organizations in the newly formed District Longleng have decided to work together under the Co-ordination of Phom Baptist Christian association and Phomla Hoichem (Phom Women’s Association). Different organizations in Noklak belonging to Khiamniungan community have formed a joint action committee to take step for prevention of HIV and care and support of infected persons. The meeting participants appreciated these efforts and discussed several others issues concerning HIV/AIDS and strategies for appropriate intervention. The concluding remark by Mr. Gunashekar, Consultant FHI, were that he would do his best to present the actual issues at stake and assured that the concerned shared by all will be presented accurately in the situation assessment and this report would reach all key stakeholders at different levels. A set of resolution passed by the meeting is listed below:
Resolutions:
The house comprising of the Tuensang Mon People’s Organization, Chang, Sangtam, Phom, Khiamniungan, Yimchunger Tribal Hohos, Tuensang Mon Students Org., Associations and Churches, GB`s, DBs, Tuensang Town Baptist women Union, Muslim and Hindu Community, District Administration, School authorities and the Police unanimously resolved to render full support to the cause of HIV people and the campaign initiated by ECS.
One key phrase by a tribal was “We request all to test and that all found positive to open-up without hesitation because we want to help you and stand by you…”.

The TMPO resolved to request the Govt. for CD4 count machine and ART therapy for Tuensang and also to establish VCTC, STD Clinic and in Longleng, Noklak, Kipheri Longkhim and Shamator Towns.
The TMPO to resolve the key pertaining to the problem of HIV/AIDS and to device strategies to tackle the same during the forth-coming session to be held in may 2004.
All tribal councils to have quarterly monitoring review sessions in their tribal sub-division with all departments to ensure cross departmental/sector collaboration to create maximum awareness in the district.
The house also resolved that ECS should provide updated statistics of the prevalence according to the tribe and sub-divisions to the tribal bodies.
Each tribal Council also resolved to pursue further thought to the on-going discussing on harm reductions measures such as needle exchange programmes and to promote easy access by all, particularly injecting drug user and to formulate policies.
The house urged the Govt. and donor agencies to provide sustained support for longer period for different prevention and care intervention. Minimum intervention period of 5 to 10 years should be considered.
The Stakeholders from different sections of society who participated actively in the meeting are listed below:
- 1. Mr.Tsubongse, Chairman, TMPO.

- 10. Mr. N. Henyei Shukha, Phom Baptist Churches Association.

- 22. Mr. K. Menya, Chairman, KTC, Noklak.

- 26. Mrs. B. Achetla Ao, Asst. Comdt, 3rd NAP.

7. Recommendations
to be written by Gunashekar